

What and why
Owing to global usage trends, Levemir® (insulin detemir), in both its Penfill® and FlexPen® presentations, is to be discontinued, with an anticipated supply end date of December 2026. A Medicine Supply Notification (MSN/2025/036U) has been issued regarding the discontinuation.
The Association of British Clinical Diabetologists (ABCD) and the Primary Care Diabetes & Obesity Society (PCDOS) have published joint guidance from a multidisciplinary team of healthcare professionals, to support clinicians in appropriately selecting and safely prescribing alternative insulin therapies (Newland-Jones et al, 2026).
The guidance was updated in May 2026 to account for the unavailability of Abasaglar® for switching and very limited extra supply of Humulin I®.
This Need to know is derived from the joint guidance and provides a brief summary for application in primary care clinical reviews, with a focus on people living with type 2 diabetes.
Background
● There are no direct alternatives to Levemir (insulin detemir), which is the only analogue basal insulin licensed for twice daily use.
● Alternative insulins need consideration, close monitoring and adjustment.
● When switching between insulins, there can be differences between absorption, potency and action profile; therefore, always consider reducing doses by 10–20% to avoid any initial risk of hypoglycaemia.
Note
The ABCD/PCDOS joint guidance should be used alongside the relevant NG28 guideline (NICE, 2026). It does not override the responsibility of the clinician to make decisions appropriate to the circumstances of the individual, in consultation with them and/or their families, carers or guardians. Responsibility remains with the prescribing clinician/clinical team.
Who should be reviewed by specialist teams?
Clinical review should be by a healthcare professional with appropriate competence in insulin/diabetes management. While this might be in primary care, the following groups should ideally be reviewed by a specialist team.
- People with allergies to alternative insulins (local allergy or diabetes services).
- Children or adolescents (any type of diabetes).
- Adults on Levemir insulin with type 1 diabetes* (includes those using insulin pumps with Levemir as backup injections).
- People with type 3c diabetes.*
- People with cystic fibrosis-related diabetes.
- Adults with type 2 diabetes on Levemir insulin with an eGFR <30 mL/min/1.73 m2.
- For people who do not wish to be referred to the specialist diabetes team, support for switching should be sought through Advice and Guidance routes.
*For people with type 1 or type 3c diabetes, it is vital to maintain consistent 24-hour basal insulin coverage. Failure to do so will increase the likelihood of diabetic ketoacidosis.
Clinical review
Explain. Explain the need to change the current diabetes management/medication plan and ensure shared decision-making throughout the review/consultation.
Assess risk factors for glucose instability. Glucose instability is a potential risk during any switch to an alternative insulin/therapy. It is particularly pertinent in the following coexisting conditions. Therefore, assess for:
- Impaired hypoglycaemia awareness.
- A history of severe hypoglycaemia.
- Any evidence of lipohypertrophy at injection sites.
- Frailty and/or older age.
- Renal or severe hepatic impairment.
- High glucose variability on CGM (if eligible to use).
- Cognitive or functional impairment.
- Learning difficulties and/or low health literacy.
- Visual impairment and/or manual dexterity problems.
- High alcohol intake or binge drinking.
- High levels of physical activity.
Current insulin regimen. Establish current dose(s) of insulin and which device is being used. Establish timing of injection(s).
Injection technique. Review injection technique (including storage of insulin) and examine for any areas of lipohypertrophy.
Individualised glucose targets. Look to set appropriate individualised target glucose levels based on, for example, comorbidities, frailty, early-onset type 2 diabetes or pre-conception planning.
Assess glucose profile. Do not use HbA1c, as this will give only a historical context and will not reveal day-to-day or in-day variability. As a minimum, four capillary blood glucose readings per day (before meals and before bed) should guide decisions. For example:
- If the blood glucose profile is generally stable, a peakless insulin will be a preferable option.
- If the blood glucose profile is peaking at a particular time of day, an insulin with a defined peak of action, with administration timed so that the peak of action corresponds with the raised blood glucose, may be more suitable.
- If nocturnal hypoglycaemia is considered to be a risk, a basal insulin with a shorter duration of action, taken once a day in the morning, may be a suitable option.
- If the blood glucose pattern is erratic or inconsistent, assess for significant variation in daily living and health behaviours (e.g. activity and sport, diet, missed insulin doses and variations in timing of insulin administration). A longer-acting basal analogue insulin may offer more flexibility with timing, or a twice-daily basal regimen with the option to adjust the doses for planned activity/sport. Alternatively, a premixed insulin taken once or twice a day with food might be more suitable.
Assess hypoglycaemia. Assess for any hypoglycaemia using open-ended questions, and confirm level of hypoglycaemia awareness.
Consider non-insulin therapies. Assess whether the current insulin regimen for type 2 diabetes could be optimised by incorporating non-insulin therapies per NICE NG28 guidance.
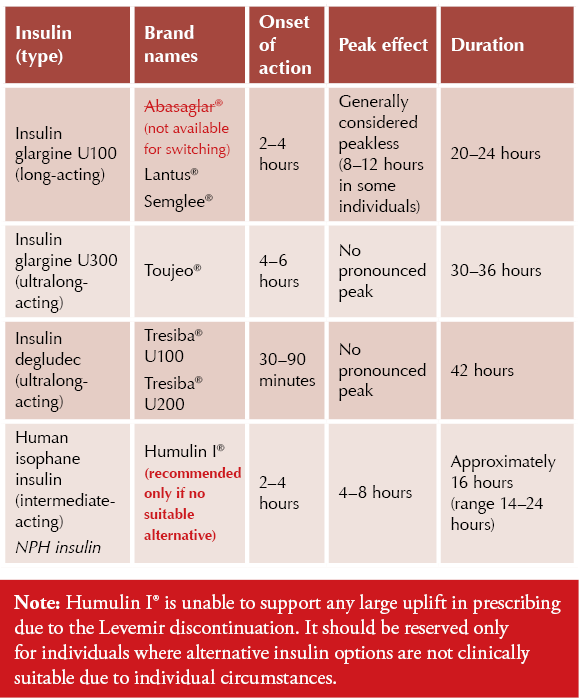
Alternative basal insulins
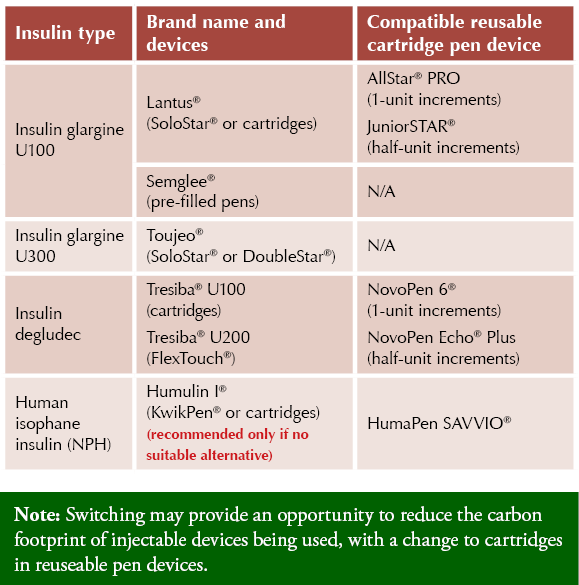
Insulin devices
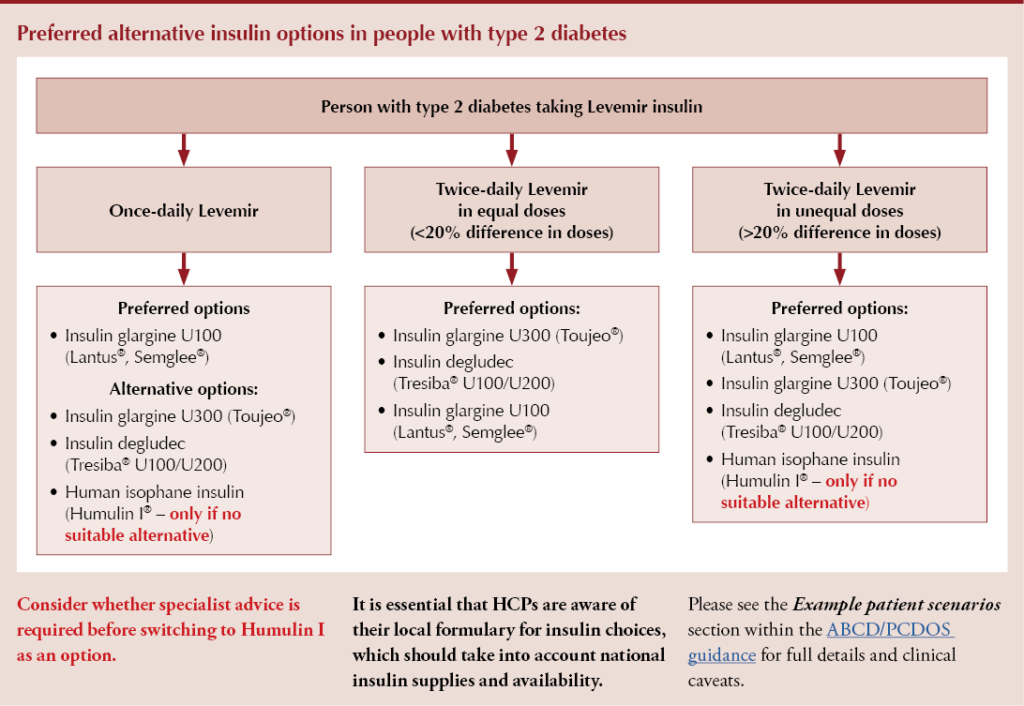
Preferred alternative insulin options in people with type 2 diabetes
Considerations when switching, with examples
Switching from once-daily Levemir
Consider reducing the dose by 10–20%, depending on fasting glucose levels and any incidence of hypoglycaemic episodes.
Example:
Levemir 30 units once daily at night, switching to insulin glargine U100 (Lantus or Semglee) once daily, could be converted to:
- 10% reduction = Lantus 27 units once daily at night.
- 20% reduction = Lantus 24 units once daily at night.
If given in the morning to avoid overnight hypoglycaemia, an intermediate-acting insulin such as Humulin I may be the most appropriate – only if there is no other suitable alternative. Consider whether specialist advice is required before switching to Humulin I as an option.
Example:
Levemir 20 units once daily in the morning being used to avoid overnight hypoglycaemia, switching to Humulin I once daily, could be converted to:
- 10% reduction = Humulin I 18 units in the morning.
- 20% reduction = Humulin I 16 units in the morning.
Notes: As with any insulin regimen, it is important to reinforce safe titration to achieve agreed blood glucose target ranges. If there is any uncertainty, seek Advice and Guidance, or refer to community/specialist diabetes services per locally agreed pathways.
Switching from twice-daily Levemir with equal doses (less than 20% difference between two doses)
If <50 units total daily dose, consider once-daily insulin glargine U100 (Lantus, Semglee). The dose would be calculated as per the worked examples below.
If the total daily dose exceeds 80 units, then the Toujeo DoubleStar device (insulin glargine U300) should be prescribed. An even number of units should be prescribed, owing to the 2-unit increments on the pen device.
- Clinical trials show that when switching to Toujeo, achieving comparable glucose control often requires a 10–18% higher dose. Therefore, while a cautious dose-reduction approach is recommended initially, it is expected that the final Toujeo dose will likely exceed the equivalent unit dose of Levemir.
Example 1:
Levemir 20 units twice daily (morning and night), switching to Toujeo, Tresiba or U100 insulin glargine (Lantus, Semglee) once daily, could be converted to:
20 units twice daily = 40 units total daily dose.
- 10% reduction = 36 units Toujeo/Tresiba/U100 glargine once daily, in the morning or night.
- 20% reduction = 32 units Toujeo/Tresiba/U100 glargine once daily, in the morning or night.
Example 2:
Levemir 18 units in the morning and 15 units at night could be converted to:
18 units morning and 15 units night = 33 units total daily dose.
- 10% reduction = 30 units Tresiba/Toujeo/U100 glargine once daily.
- 20% reduction = 27 units Tresiba/Toujeo/U100 glargine once daily.
Notes: As with any insulin regimen, it is important to reinforce safe titration to achieve agreed blood glucose target ranges. If there is any uncertainty, seek Advice and Guidance, or refer to community/specialist diabetes services per locally agreed pathways.
Switching from twice-daily Levemir with unequal doses (more than 20% difference between two doses)
If converting to a once-daily basal insulin, take the lowest of the two Levemir doses and multiply this by 2; consider this the maximum safe daily dose initially.
Example:
Levemir 20 units in the morning and 14 units at night, switching to insulin glargine U100 (Lantus, Semglee), Toujeo or Tresiba once daily, can be calculated as:
Maximum safe daily dose* = lowest dose Levemir × 2 (14 units × 2 = 28 units).
- 10% reduction = 25 units once daily, in the morning or night.
- 20% reduction = 22 units once daily, in the morning or night.
*A significant reduction in total daily dose using this last method may indicate future underdosing during part of the day. In such cases, adjustments to mealtime insulin (if prescribed) or to adjunct oral and injectable therapies in type 2 diabetes should be considered. As with any insulin regimen, it is important to look to reinforce safe titration to achieve agreed blood glucose target ranges.
Switch to Humulin I only if there is no other suitable alternative. Consider whether specialist advice is required before switching.
If converting to twice-daily Humulin I, reduce each individual dose by 10–20% compared with the Levemir dose, matching the original prescribing times.
Example:
Levemir 36 units in the morning and 20 units in the evening, switching to Humulin I, can be calculated as:
- 10% reduction = Humulin I 32 units morning and 18 units evening.
- 20% reduction = Humulin I 29 units morning and 16 units evening.
Notes: As with any insulin regimen, it is important to reinforce safe titration to achieve agreed blood glucose target ranges. If there is any uncertainty, seek Advice and Guidance, or refer to community/specialist diabetes services per locally agreed pathways.
Education checklist
❑ Explain/demonstrate any new delivery device (including to family/carers as required).
❑ Reinforce insulin injection technique and provide for any adjustments as required.
- If lipohypertrophy is detected, considerable dose adjustment is often required when changing injection sites. Seek Advice and Guidance as necessary if unsure.
❑ Confirm insulin storage and sharps disposal.
❑ Confirm insulin dose and timing.
❑ Provide insulin “credit card-sized” safety cards, passports, booklets and/or Patient Information Leaflets.
❑ Advise on frequency of capillary glucose testing to ensure meaningful monitoring.
❑ Provide education on CGM (where eligible), to ensure effective use.
❑ Provide education and support to help individuals self-adjust their insulin dose(s).
- This may be an opportunity to signpost to diabetes education in general, either formal or informal.
❑ Provide healthy living advice, to include effects of foods and exercise on glucose levels.
❑ Ask about the person’s emotional wellbeing and assess for any diabetes distress.
❑ Recap on hypoglycaemia: Prevention, signs and symptoms, and management.
❑ Provide guidance on sick day rules, DVLA and driving rules, fasting in Ramadan and travel.
❑ Ensure those with type 1 diabetes have a blood ketone meter and in-date blood ketone test strips, and that they know how to interpret these as part of sick day rules.
❑ Ensure adequate safety-netting, advising when and how to report any concerns about glucose levels that the person may have.
❑ Arrange for a review at 2–3 weeks, to continue to support with dose titration as necessary, and to review the suitability of the new insulin regimen.
- For those at higher risk of dysglycaemia, aim for close clinical review within 1–2 weeks of change where possible.
Useful resources
● Leicester Diabetes Centre: Insulin Therapies: An Educational Toolkit
● American Diabetes Association: Pharmacologic approaches to glycemic treatment: Standards of Care in Diabetes
● Free e-Learning module: The Six Steps to Insulin Safety
● Trend Diabetes: Injection Technique Matters resources
● Diabetes & Primary Care: Insulin guides series
Acknowledgement
The authors thank Philip Newland-Jones for leading on the joint guidance and providing feedback on this article.
More support
In this video, the PCDO Chairs are joined by Philip Newland-Jones to discuss the guidelines and how to implement them.



Guest Editor Hannah Beba asks which outcomes – beyond mere numbers – are most important to the individual, the clinician and the NHS.
7 Jul 2026