

What and why
The Drivers’ Medical Section within the DVLA deals with all aspects of driver licensing when there are medical conditions that impact, or potentially impact, safe control of a vehicle.
A driver can be fined up to £1000 if they fail to notify the DVLA about a medical condition that affects their driving and may be prosecuted if they are involved in an accident as a result.
This summarises guidance for healthcare professionals (HCPs) based on the November 2025 update of Assessing Fitness to Drive, available here.
Doctors and other healthcare professionals should:
- Advise the individual on the impact of their medical condition on safe driving ability.
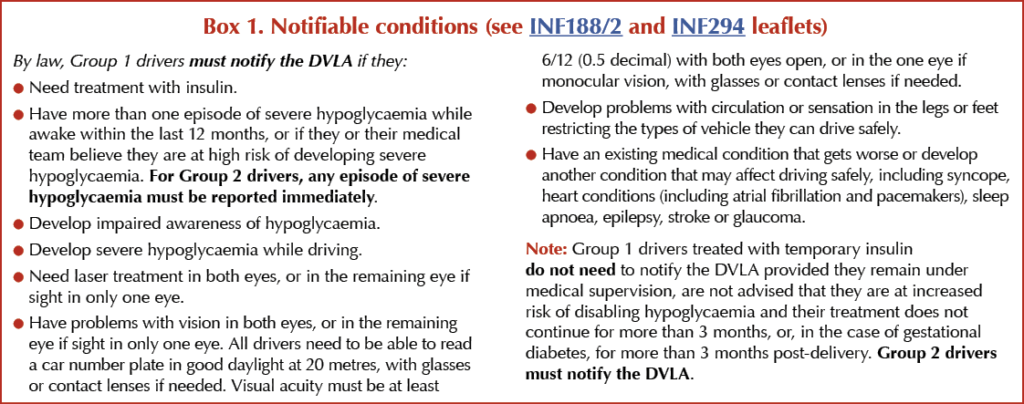
- Advise the individual of their legal requirement to notify the DVLA of any relevant condition, or if they meet the notification criteria in Box 1 or start insulin therapy.
- Provide the information leaflets INF188/2 for drivers treated with non-insulin medications, diet or both; INF294 for those treated with insulin; and INS186 for those wishing to apply for Group 2 entitlement.
- Notify the DVLA directly of an individual’s medical condition or fitness to drive if they cannot or will not notify the DVLA themselves (see GMC guidance on confidentiality and reporting to the DVLA).
HCPs should always record in their consultation notes that advice has been provided regarding driving and diabetes, especially with respect to fitness to drive, hypoglycaemia risk and appropriate glucose monitoring.
All HCPs who provide guidance on diabetes should familiarise themselves fully with chapter 3 of Assessing Fitness to Drive and other sections as appropriate, and discuss with colleagues or the DVLA Medical Team if they are uncertain about how to interpret guidance in relation to individual patients.
Assessing fitness to drive
| Group 2 drivers (large lorries [category C] and buses [category D]) In most cases, the medical standards for Group 2 drivers are substantially higher than for Group 1 (car and motorcycle) drivers. This is because of the size and weight of the vehicle and the length of time an occupational driver typically spends at the wheel. Note: Drivers with a Group 1 category B licence issued before 1 January 1997 have additional driving entitlements until the licence expires or is revoked for medical reasons: see here. Taxi and emergency vehicle drivers The DVLA states that the same medical standards apply for drivers of taxis and police, fire, coastguard, ambulance and health service vehicles as for drivers of regular vehicles. However, individual forces, services or council licensing bodies may impose higher medical standards over and above these licensing requirements. |
Diabetes treated by diet or lifestyle alone
| Group 1 Car and motorcycle | Group 2 Bus and lorry |
| May drive and need not notify the DVLA, provided the driver meets the requirements in leaflet INF188/2. Must have no disqualifying complications of diabetes. | May drive and need not notify the DVLA, provided the driver meets the requirements set out in leaflet INF188/5. Must have no disqualifying complications of diabetes. |
Diabetes treated by medication other than insulin
| Group 1 Car and motorcycle | Group 2 Bus and lorry | |
| Managed by tablets carrying hypoglycaemia risk (includes sulfonylureas and glinides) | May drive and need not notify the DVLA, provided the driver: ● Has adequate awareness of hypoglycaemia (being able to recognise symptoms in time to safely stop the vehicle). ● Has not experienced two or more episodes of severe hypoglycaemia while awake in the last 12 months and the most recent episode occurred more than 3 months ago. ● Is under regular review. ● Has no disqualifying complications of diabetes. It is advisable to practise appropriate glucose monitoring at times relevant to driving to enable the detection of hypoglycaemia. If required, notify DVLA by completing form DIAB1. | May drive but must notify the DVLA. All the following criteria must be met for DVLA to issue a licence for 1, 2 or 3 years: ● No episode of severe hypoglycaemia in the last 12 months. ● Full awareness of hypoglycaemia. ● Regular self-monitoring of glucose – at least twice daily and at times relevant to driving, such as at the start of the first journey and at least every 2 hours during the journey (CGM is accepted but must also carry a fingerprick meter as a backup). ● Demonstrates an understanding of the risks of hypoglycaemia. ● Under regular medical review. ● Has no disqualifying complications of diabetes. If required, notify DVLA by completing form VDIAB1SG. |
| Managed by other medications (includes metformin, DPP-4is, SGLT2is, GLP-1 RAs and non-insulin injectables) | May drive and need not notify the DVLA, provided the requirements set out in leaflet INF188/2 are met and the driver is under regular medical review. Must have no disqualifying complications of diabetes. If required, notify DVLA by completing form DIAB1. | May drive but must notify the DVLA. DVLA may issue a licence if the requirements set out in leaflet INF188/2 are met and the driver is under regular medical review. Must have no disqualifying complications of diabetes. If required, notify DVLA by completing form VDIAB1GEN. |
Diabetes treated by insulin
By law, people treated with insulin must inform the DVLA immediately.
| Group 1 Car and motorcycle | Group 2 Bus and lorry |
| Must notify the DVLA if: ● Insulin treatment lasts (or will last) over 3 months. ● Following gestational diabetes, insulin treatment lasts over 3 months after the birth. ● Person gets disabling hypoglycaemia or is at risk of developing it. Report condition online at: https://www.driving-medical-condition.service.gov.uk/report or complete form DIAB1. Read leaflet INF294. All the following criteria must be met for DVLA to license the person with insulin-treated diabetes for 1, 2 or 3 years: ● Adequate awareness of hypoglycaemia (being able to recognise symptoms in time to safely stop the vehicle). ● Has not experienced two or more episodes of severe hypoglycaemia while awake in the preceding 12 months and the most recent episode occurred more than 3 months ago (see Recurrent severe hypoglycaemia guidance). ● Practises appropriate glucose monitoring as defined below. ● Not regarded as a likely risk to the public while driving. ● Meets the visual standards for acuity and visual field. ● No disqualifying complications of diabetes. ● Under regular medical review. | Must stop driving and notify the DVLA when insulin treatment is started. Complete form VDIAB1I. Read leaflet INS186 to find out how to get a licence to drive large vehicles if diabetes is treated with insulin. Before starting a driving licence application, the person must have had a stable medical condition for at least one month. DVLA will advise as to when Group 2 driving is permitted again. All the following criteria must be met for DVLA to license the person with insulin-treated diabetes for 1 year (with annual review): ● Full awareness of hypoglycaemia (symptoms when glucose falls below 3.5 mmol/L). ● No episode of severe hypoglycaemia in the preceding 12 months. ● Practises glucose monitoring with the regularity defined below. ● Must use a glucose meter with sufficient memory to store 4 weeks of readings, or accurate CGM, as detailed below. ● Demonstrates an understanding of the risks and symptoms of hypoglycaemia. ● No disqualifying complications of diabetes that would mean a licence being refused or revoked, such as visual field defects. ● Under regular medical review. ● No other conditions that preclude driving. |
Glucose self-monitoring requirements
| Group 1 Car and motorcycle | Group 2 Bus and lorry |
| For those using a capillary glucose monitor, testing must take place: ● At the start of the first journey. ● At least every 2 hours during the journey. A maximum of 2 hours should pass between the pre-driving glucose test and the first glucose check performed after driving has started. More frequent self-monitoring may be required with any greater risk of hypoglycaemia (such as physical activity or altered meal routine). For those using CGM: ● The device must be approved for adjunctive use (see below). ● Must have a backup capillary glucose meter. Applicants will be asked to sign an undertaking to comply with the directions of the healthcare professionals treating their diabetes and to report any significant change in their condition to DVLA immediately. Applicants should know how to respond if hypoglycaemia occurs when driving (see Advice for drivers section). | For those using a capillary glucose monitor, testing must take place: ● At least twice daily, including on days when not driving. ● At the start of the first journey. ● At least every 2 hours during the journey. A maximum of 2 hours should pass between the pre-driving glucose test and the first glucose check performed after driving has started. More frequent self-monitoring may be required with any greater risk of hypoglycaemia (e.g. physical activity or altered meal routine). A bus or lorry driver may be licensed if they need to use more than one glucose meter with a memory function to ensure that 4 weeks of readings while on insulin are available for assessment. For those using CGM: ● The device must be approved for adjunctive use (see below). ● Must use CGM at least 70% of the time (preferably >90%). ● Must have alarms set at >4 mmol/L. ● Must have a backup capillary glucose meter. To ensure the requirements are met for the licensing of insulin-treated Group 2 bus and lorry drivers, applicants must: ● Attend an examination every 12 months by an independent consultant specialist in diabetes. At the examination, the consultant will require sight of CGM or capillary glucose records: ➤ For capillary glucose monitors, the assessor requires a minimum of 56 readings over the past 28 days. ➤ For CGM, the assessor requires 30 days of CGM data to confirm the rules above, and that Time Below Range is <10%. Applicants will be asked to sign an undertaking to comply with the directions of the healthcare professionals treating their diabetes and to report any significant change in their condition to the DVLA immediately. Applicants should know how to respond if hypoglycaemia occurs when driving (see Advice for drivers section). |
Continuous glucose monitoring (CGM) systems
In November 2025, the DVLA issued changes that allow Group 2 drivers with diabetes to use CGM systems to monitor their glucose levels for the purpose of driving. This brings them in line with Group 1 drivers, who have been allowed to use this technology since 2018.
CGM may be used for monitoring glucose at times relevant to driving, but users must also carry fingerprick capillary glucose testing equipment as backup. This is essential in case the CGM stops working or gives readings that do not match how the person feels (e.g. symptoms of hypoglycaemia but no low reading shown).
Device alarms are a helpful tool but should not replace the individual’s own awareness of low glucose symptoms or regular self-checks.
A capillary blood glucose reading must be taken in the following circumstances:
- When blood/interstitial glucose is 4.0 mmol/L or below.
- When symptoms of hypoglycaemia are being experienced.
- When the glucose monitoring system gives a reading that is not consistent with the symptoms being experienced.
Drivers should use a device that is medically approved for non-adjunctive use, meaning it is approved for making insulin treatment decisions based on CGM readings. This ensures the monitor meets the required safety and quality standards. A list of monitors approved for non-adjunctive use is available from the DSN Forum.
Recurrent severe hypoglycaemia guidance
The law defines “severe” as an episode of hypoglycaemia requiring the assistance of another person.
● For Group 1 drivers, hypoglycaemia that happens during established sleep is no longer considered relevant for licensing purposes, unless there are concerns about the driver’s ability to recognise low glucose.
- Group 1 drivers who have had two or more episodes of severe hypoglycaemia while awake in the last 12 months must not drive and must notify the DVLA. DVLA will then carry out medical enquiries before a licensing decision is made.
● Group 2 drivers must stop driving after any episode of severe hypoglycaemia requiring the help of another person (occurring at any time, including during sleep) and report all episodes to the DVLA.
● All Group 1 and Group 2 drivers who experience an episode of severe hypoglycaemia whilst driving must stop driving immediately and must notify the DVLA.
Impaired awareness of hypoglycaemia
Impaired awareness of hypoglycaemia is defined as being unable to recognise when blood glucose levels are low or starting to fall, due to a total absence of warning symptoms.
The Secretary of State’s Honorary Medical Advisory Panel on Driving and Diabetes defines adequate awareness of hypoglycaemia as being able to recognise symptoms in time to safely stop the vehicle.
Group 2 drivers must have full awareness of hypoglycaemia.
The alarms on glucose monitoring devices should supplement, not replace, the individual’s own awareness and active self-monitoring practices, and should be set at appropriate levels of above 4.0 mmol/L while driving. If a driver becomes dependent on these alarms to recognise low glucose, they must stop driving and notify the DVLA.
Complications that may affect fitness to drive
Drivers with these complications may need to stop driving and must notify the DVLA:
Visual complications
- Minimal standards – see Box 1 – for acuity and number plate reading. Field of vision of at least 120 degrees horizontal, including 50 degrees left and right.
- Monocular vision – must meet same visual standards; may only drive after clinical advice of successful adaptation to the condition.
- Visual field defects (including glaucoma and retinopathy/treatment for retinopathy) – must notify DVLA and meet criteria for driving. Guidance is complex – consult chapter 6 of Assessing Fitness to Drive and ensure formal visual field testing if appropriate.
Excessive sleepiness, including obstructive sleep apnoea (even before formal diagnosis)
Guidance based on apnoea/hypopnoea index (AHI) and sleepiness:
● AHI <15 per hour/mild, or excessive sleepiness – must not drive until satisfactory symptom control; must notify DVLA if symptom control not achieved in 3 months.
● AHI 15–29 per hour/moderate, with sleepiness; or AHI >30 per hour/severe, without sleepiness; or suspected diagnosis – must not drive and must notify DVLA. Licensing will require control of condition, sleepiness improved, treatment adherence confirmed medically; must agree to 3-year review.
● Group 2 drivers: if any suspicion of OSA, must not drive until diagnosis and symptoms are proven to be under control.
● See also guidance on hypersomnias including narcolepsy.
Renal complications
Ambulatory dialysis or haemodialysis:
Group 1: only notify if severe electrolyte disturbance or complications (e.g. sudden attacks of disabling dizziness or fainting, impaired psychomotor or cognitive function).
Group 2: must notify DVLA.
Limb complications, including peripheral neuropathy
See Appendix F of Assessing Fitness to Drive.
Hypoglycaemia due to other causes
Group 1 and 2 drivers – if episodes of severe hypoglycaemia from any cause (e.g. post-bariatric surgery or related to eating disorders), driving must stop while liability to episodes remains.
Pancreas or islet cell transplants
● Group 1 drivers – may drive but must notify DVLA. Licensing only if no disqualifying conditions. If on insulin, follow Group 1 insulin guidance.
● Group 2 drivers – may drive but must notify DVLA. Licensing will require individual assessment. If on insulin, follow Group 2 insulin guidance.
Advice for drivers
Glucose monitoring
● Carry a fingerprick blood glucose meter and testing strips (must be in date/not expired) in your car.
- Carry spares, including test strips, lancets and batteries.
● If using continuous glucose monitoring (CGM), use a CGM device that is medically approved for non-adjunctive use (approved for treatment decisions based on CGM readings alone) – see the DSN Forum guide.
● Use a fingerprick monitor to confirm your glucose level if your CGM device or sensor isn’t working, or if your CGM reading doesn’t match how you feel.
● Trust your symptoms – don’t rely solely on CGM if you feel unwell. Note: device alarms are a helpful tool but they should support, not replace, your own awareness of low blood glucose symptoms or regular self-checks.
● Carry ID showing you have diabetes in case of an accident.
Avoiding and responding to hypoglycaemia
● Check your glucose level before driving, and on long journeys stop every 2 hours to recheck. If blood glucose is less than 5 mmol/L, do not drive.
- If your glucose is between 4.0 mmol/L and 5.0 mmol/L, eat a fast-acting carbohydrate snack before driving.
- If your glucose is less than 4.0 mmol/L, treat the hypoglycaemia and wait at least 45 minutes until after glucose levels return to at least 5.0 mmol/L.
- Do not drive if feeling hypoglycaemic.
● If hypoglycaemia develops while driving, stop driving as soon as possible in a safe location, switch off the engine, remove keys from the ignition and move from the driver’s seat.
- Treat the hypoglycaemia and do not resume driving until 45 minutes after glucose has returned to at least 5.0 mmol/L.
● Keep an emergency supply of fast-acting carbohydrate, such as glucose tablets or sweets, within easy reach in the vehicle.
● Take regular meals, snacks and rest periods on long journeys, and always avoid alcohol.
● Take extra care during changes of insulin regimens, changes of lifestyle, exercise, travel and pregnancy.
Motor insurance
● Drivers must declare that they have diabetes when applying for insurance.
- Most car insurers do not charge higher premiums for people with diabetes. If the drivers feel they are being discriminated against, they can complain to the insurance company or switch to a new company.
- See Diabetes UK’s Insurance and diabetes for more information.
● See driving advice at Diabetes UK’s Driving and diabetes and Trend Diabetes’s Safe Driving and the DVLA.
List of resources
For healthcare professionals
● DVLA: Assessing fitness to drive: a guide for medical professionals – https://bit.ly/4dwKY1b
● GMC: Confidentiality: patients’ fitness to drive and reporting concerns to the DVLA or DVA – https://bit.ly/3PQS2vV
● DSN Forum: CGM systems for insulin dosing comparison charts – https://bit.ly/4cyVgNi
● Diabetes & Primary Care: At a glance factsheet: Impaired hypoglycaemia awareness – https://bit.ly/3Ow0ikq
For people with diabetes: information leaflets
● DVLA: A guide to insulin treated diabetes and driving (INF294) – https://bit.ly/3QaChjm
● DVLA: Information for drivers with diabetes treated by non-insulin medication, diet, or both (INF188/2) – https://bit.ly/4cDyBhV
● DVLA: Lorry and bus drivers with diabetes treated by diet alone: When do you need to tell us? (INF188/5) – https://bit.ly/4e711D6
● DVLA: A guide for drivers with insulin treated diabetes who wish to apply for lorry or bus entitlement (Group 2) (INS186) – https://bit.ly/4mmeh8X
● Diabetes UK: Driving and diabetes – https://bit.ly/4ebvcsM
● Diabetes UK: Diabetes and your driving licence – https://bit.ly/4em6sy5
● Trend Diabetes: Diabetes: Safe driving and the DVLA – https://bit.ly/4mkv38n
For people with diabetes: DVLA reporting forms
● Form DIAB1 (for Group 1 drivers) – https://bit.ly/3O9SODG
● Form VDIAB1SG (for Group 2 drivers treated with sulfonylureas or glinides) – https://bit.ly/47ShFm6
● Form VDIAB1GEN (for Group 2 drivers treated with non-insulin injectables or tablets other than sulfonylureas or glinides) – https://bit.ly/3PZlhg3
● Form VDIAB1I (for Group 2 drivers treated with insulin) –
https://bit.ly/4dBYJvF
Acknowledgement
The author thanks Pratik Choudhary for his support in clarifying changes to the guidance.



Guest Editor Hannah Beba asks which outcomes – beyond mere numbers – are most important to the individual, the clinician and the NHS.
7 Jul 2026