

What and why
There is limited evidence for the use of specific carbohydrate counting in type 2 diabetes care outside of those people on a basal–bolus insulin regimen. However, a lack of direct evidence is not evidence of lacking.
The breadth of information people are exposed to regarding food types, patterns and how specific nutrients may or may not affect their health is vast. The influence of unverified or misrepresented statements on the internet or media often means people visit us with questions and confusion, and it can be difficult to know where to start or what to cover.
This tiered approach to carb counting in type 2 diabetes is based on clinical experience, aligned with available evidence, patient feedback and outcomes which, taken together, highlight that carbohydrate education, including carbohydrate counting for appropriate people, continues to play an important role in holistic type 2 diabetes care. Individualised management is key.
This is not a guideline to be followed strictly, but is instead a sharing of best practice and a clarification of what to discuss with the heterogeneous populations of people with type 2 diabetes we see.
Why is carbohydrate awareness important?
There is no recommended daily volume of carbohydrate for someone with type 2 diabetes to consume. However, a reduction from their current intake will reduce glycaemic load and thus support blood glucose management.
If some carbohydrate is replaced by protein and/or high-fibre foods, this can further benefit in the context of lean mass retention and cardiovascular risk.
Carbohydrate identification and awareness often leads to carbohydrate reduction, which can both reduce glycaemic load and support weight loss, and often improves dietary protein and fibre intake as well. Weight management remains a primary lifestyle component in type 2 diabetes, with evidence suggesting that the majority of people with type 2 diabetes would benefit from some degree of weight loss.
Pragmatic wins
Protein and fibre. Additional dietary protein and fibre have well-established benefits on weight management, satiation, muscle mass support, colorectal cancer (fibre only), all-cause mortality and glycaemic management.1–3 Alongside encouraging people to reduce carbohydrate intake, we should recommend the following, either individually or in combination:
● Replacement with protein: recommended target of 1.2–1.6 g per kg ideal bodyweight per day, or 20–30 g protein with each main meal.
● Replacement with fibre: 20–25 g per 1000 kcal consumed, or 30–35 g per day.
Encourage people to increase protein and fibre intake gradually and to encourage even small changes. The numbers provided are grounded in research but realism needs to be considered (e.g. cost, access to food, ability to prepare food). Protein or fibre supplements could be used if convenient and cost-effective, and can markedly improve the nutrient profile of a person’s diet when used appropriately.
Portion plate. This is a low-burden, easily adopted option for people. It is generally well received for its simplicity and shows comparable efficacy in glycaemic outcomes to formal carbohydrate education/awareness.
Split the plate into three sections:
- ½ fibrous vegetables.
- ¼ carbohydrates.
- ¼ protein source.
Weight and glycaemia. For meaningful improvements in glycaemia, any macronutrient manipulations need to be sustainable and, for maximum impact, support weight loss outcomes. Weight loss remains the most effective intervention for improving blood glucose levels.4,5
A tiered approach to carbohydrate counting education for type 2 diabetes
The majority of people with type 2 diabetes are likely to benefit from at least some degree of carbohydrate awareness (refer to How to improve carbohydrate awareness for more specific detail).
However, for more advanced carbohydrate education, and as part of the shared decision-making process, different approaches may be required depending on the individual’s current stage of their diabetes journey, motivation levels, treatment regimen, numerical literacy, general education and cultural influences, for example.
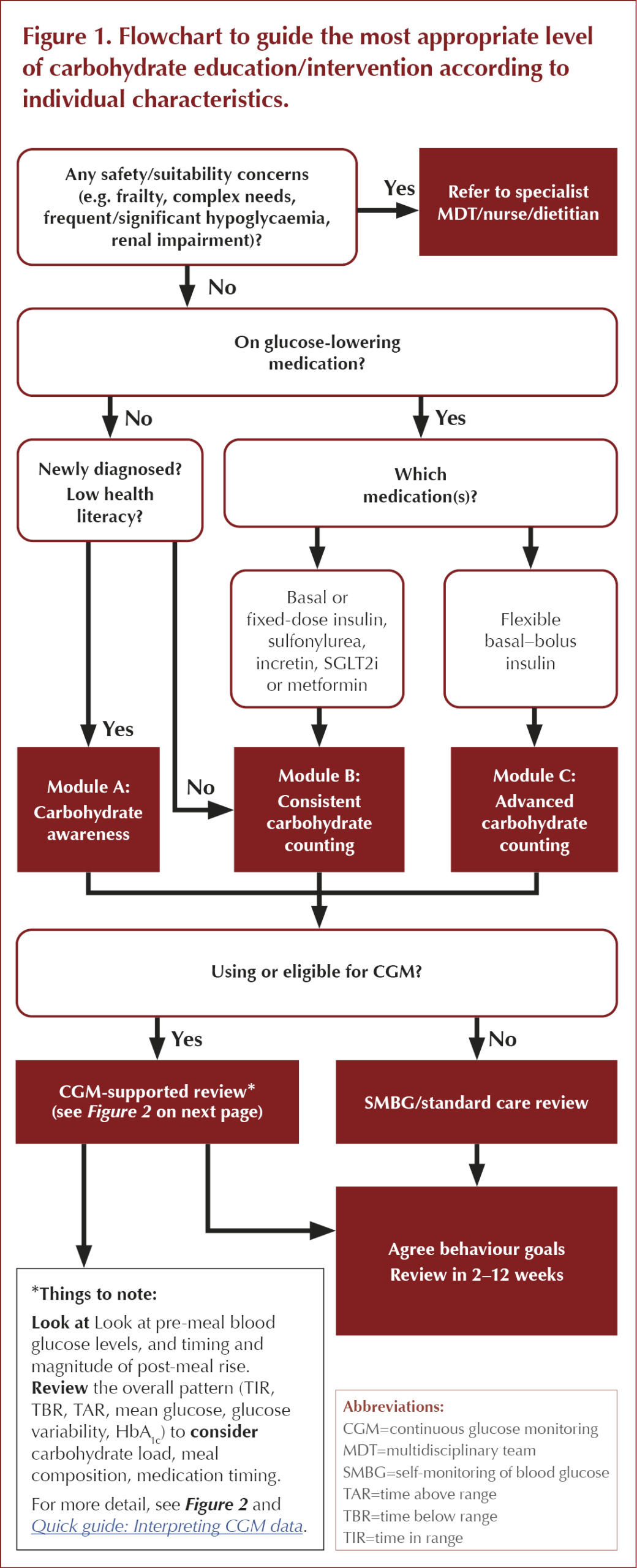
The tiered approach to carbohydrate education in type 2 diabetes described overleaf recommends three levels of carbohydrate education/intervention according to the individual’s circumstances.
● Module A supports people to develop a foundational knowledge of identifying and understanding carbohydrates.
● Module B covers the most likely interpretation of “carbohydrate counting” for type 2 diabetes outside of basal–bolus insulin regimens, with a focus on reduction and consistency.
● Module C is for people taking basal–bolus insulin regimens or highly motivated individuals. The greater variability of insulin resistance displayed in people with type 2 diabetes means calculation of ratios differs to standard type 1 diabetes practices; thus, support from a diabetes specialist nurse or multidisciplinary team will be required.
- Disclaimer: It is outside the scope of this guide to discuss specific insulin ratios for people with type 2 diabetes, particularly given the range of other medications many people will be on. This is something to be discussed with the wider multidisciplinary team/medication prescribers.
How to use
Use Figure 1 to establish which nutrition information module would best suit the individual. Each module provides areas of advice to focus on, plus the aims of that module in relation to the person’s care. Module B provides more specific detail of pragmatic, evidence-based topics to use as a framework to then structure more individualised patient advice.
- Note: It may be that there is overlap between module content covered in a single consultation. Each module acts as a guide, with Module A being the most foundational, but the three do not need to be considered totally separate.
Use Figure 2 to focus on specific areas of a CGM report based on the person’s data (if applicable), with suggestions as to how health behaviours and medication may be adjusted. Medication changes will need discussion with relevant healthcare professionals.
Module A: Carbohydrate awareness
1. Identify carbohydrate-containing foods (e.g. pasta, potato, rice, bread, sugar, honey, fruits/fruit juice, milk, cereals, pulses).
2. Label reading basics (total carbohydrate – not just “of which sugars”).
3. Impact of carbohydrate portions on blood sugars (reducing carbohydrate load and avoiding multiple sources per meal will lessen blood glucose rises).
4. Impact of type of carbohydrate on blood sugars (those containing more fibre or other nutrients [e.g. wholemeal options, whole fruits, pulses] will likely lessen or slow blood sugar rises).
Aims:
- Early improvements in HbA1c.
- Reduction in post-meal glucose rises.
- Develop confidence and autonomy.
Module B: Consistent carbohydrate counting
1. Maintain regular meal timings/patterns
2. Consistent carbohydrate portions at each meal
- Portion plate:
- ½ fibrous vegetables.
- ¼ carbohydrates.
- ¼ protein source.
- Aim for consistency of portions when having bread, potatoes, pasta, rice, etc.
3. Reduction of carbohydrate from current amount
- Encourage even small changes (e.g. reducing from two slices of bread to one, or from ¾ of a bowl of rice or cereal to ½ a bowl).
4. Nutrient interactions
- Identify and support foods with higher protein and fibre in place of carbohydrate:
- Protein: Aim to increase to 1.2–1.6 g per kg ideal body weight per day, or 20–30 g protein with each meal (3 meals per day pattern). Promote lean meat, oily fish, eggs, quorn, tofu, low-fat strained yoghurt.
- Fibre: Aim for 20–25 g per 1000 kcal consumed, or 30–35 g per day (increase gradually from current level). Promote wholegrain versions of breads and cereals, whole fruits and vegetables, lentils, chickpeas.
Aims:
- Consistent post-meal glucose reductions/patterns.
- Improvements in HbA1c.
- Complement medication/medical management.
- Support weight management aims or CVD risk reduction.
Module C: Advanced carbohydrate counting (support from diabetes MDT recommended)
1. Counting specific carbohydrate grams per meal (using previous food label understanding)
2. Insulin-to-carbohydrate ratios
- People with type 2 diabetes on basal–bolus regimens can be supported to adjust mealtime bolus doses according to the amounts of carbohydrate to be consumed, and to take activity levels into account.
- Bolus doses for standard meal types can be individualised, with support of a diabetes dietitian.
3. Correction dosing
- Adjustment of mealtime bolus insulin according to pre-meal blood glucose levels (e.g. below, within or above target ranges). Correction ratios will need support from the diabetes multidisciplinary team and are outside the scope of this guide to cover in detail.
Aims:
- Improvements in HbA1c.
- Empower and individualise management.

What does the evidence say?
Clinical glycaemic benefits and wider health outcomes from carbohydrate identification awareness, basic carbohydrate counting or even low-carbohydrate diets are, at best, modest in people with type 2 diabetes, outside of those on a basal–bolus insulin regimen. The evidence is predominantly mixed.
This is likely due to heterogeneity between individuals, including pathology of type 2 diabetes (beta-cell dysfunction, insulin resistance) and disease progression; presence of other comorbidities that may influence glucose metabolism (e.g. obesity, hyperlipidaemia); and medications, all of which make management more complex.
Carbohydrate awareness
Carbohydrate identification and awareness delivered through diabetes self-management education (DSME) shows mixed to modest improvements in glycaemic outcomes. However, wider, holistic benefits are noted from DSME, evidenced by data from DESMOND cohorts showing improvements in smoking cessation, weight management, illness beliefs and depression.6
Basic carbohydrate counting
Clinical data from basic carbohydrate counting (consistent carbohydrate and portion sizes, often using the plate method) again shows mixed HbA1c improvements, with possible reductions ranging from ~2.2 to 8.7 mmol/mol. Greater HbA1c reductions are often seen alongside weight loss.7,8
Accumulated evidence shows that the overall volume of carbohydrate (glycaemic load), dietary fibre and the quality of carbohydrates are more influential topics than glycaemic index (GI) in isolation, and they are often more practical in consultations.9,10
Low-carbohydrate diets
Lower-carbohydrate interventions (usually ≤45% of total energy intake) show mixed glycaemic benefits. Observed HbA1c reductions are on average between 3.3 and 8.7 mmol/mol, with a dose–response relationship observed (the greater the carbohydrate reduction, the greater the HbA1c improvement). However, benefits for the majority of people appear to be reduced after 6–12 months.11
Useful resources
● Diabetes & Primary Care: How to improve carbohydrate awareness
● PCDO Society e-Learning module: Continuous glucose monitoring – Introduction to time in range



Guest Editor Hannah Beba asks which outcomes – beyond mere numbers – are most important to the individual, the clinician and the NHS.
7 Jul 2026