
Diabetes in older people
Clare Hambling, GP and PCDS Chair
Later life
- Diabetes prevalence is increasing, with lifestyle factors, diet, sedentary behaviour and weight gain considered the major contributing factors. Decline in communicable disease, population growth and improving life expectancy mean that age and ageing are now recognised as risk factors for diabetes.
- The greatest age-specific rise in diabetes prevalence is expected in people ≥65 years.
- Increasing life expectancy carries with it the risk of living for more years with illness and disability. Multimorbidity is almost inevitable amongst older people with diabetes, increasing complexity of diabetes care and the likelihood of polypharmacy.
- A recent position statement from Primary Care Diabetes Europe (Hambling et al, 2019) provides a good summary.
Frailty
- Frailty is: “a medical syndrome with multiple causes and contributors, characterised by diminished strength, endurance, and physiologic function that increases an individual’s vulnerability for developing increased dependency and/or death” (Morley et al, 2013).
- The relationship between diabetes and frailty is bidirectional. Loss of muscle mass (sarcopenia) is associated with increased insulin resistance, which may exacerbate glycaemia, but poor health due to hyper- or hypoglycaemia may exacerbate muscle wasting, resulting in progressive sarcopenia.
- The Electronic Frailty Index (eFI) is a computer algorithm that generates a frailty score, which should be confirmed with clinical assessment. Use gait speed, timed get up and go test, FRAIL scale or Rockwood Clinical Frailty Scale to confirm frailty.
- Fatigue should prompt clinical assessment for underlying causes (e.g. anaemia, B12 deficiency, hypothyroidism, depression, sleep apnoea, hypotension and pharmacological causes).
- Polypharmacy is a significant contributor to frailty. Conduct a medication review, particularly looking for: medications with anticholinergic properties; drug–drug interactions; drugs altering muscle power; drug-induced hyponatraemia or dehydration; and potential overtreatment with blood-pressure or glucose-lowering medications.
Hypoglycaemia
- Older people are at increased risk from hypoglycaemia, owing to a constellation of factors, and are more likely to need hospital admission due to severe hypoglycaemia.
- Set clinically appropriate glycaemic targets based on holistic assessment:
- Fit and functionally independent: 53–59 mmol/mol.
- Complex health problems, mild/moderate frailty or fit older people on sulfonylureas or insulin: 53–64 mmol/mol.
- Very complex, poor health or frail: 59–69 mmol/mol.
- End of life: avoid symptomatic hyper- or hypoglycaemia.
- Consider the risks and benefits of the different glucose-lowering therapies when prescribing in older people.
Resources
- Talking Head: Diabetes in later life:
http://bit.ly/34yi0Xr - Hambling CE et al (2019) Factors influencing safe glucose-lowering in older people with type 2 diabetes. A position statement of Primary Care Diabetes Europe. Prim Care Diabetes 13: 330–52
- Morley JE et al (2013) Frailty consensus: a call to action. J Am Med Dir Assoc 14: 392–7
- Rockwood Clinical Frailty Scale:
https://bit.ly/2r7WCuy
Hypertension and diabetes
Patrick Holmes, GP, Darlington
- Appropriately managing hypertension in diabetes helps prevent micro- and macrovascular complications.
- NICE updated its guidance on the diagnosis and management of hypertension in adults (NG 136) in 2019.
- A diagnosis of hypertension is confirmed in people with a clinic blood pressure (BP) ≥140/90 mmHg, which is equivalent to an ambulatory BP monitoring (ABPM) daytime average or home BP monitoring (HBPM) average ≥135/85 mmHg.
- The clinic BP target for uncomplicated and non-frail individuals living with diabetes is <140/90 mmHg; if CKD aim for <130/80 mmHg.
- For those ≥80 years, the target is <150/90 mmHg.
- In individuals with type 2 diabetes, measure sitting and standing BP (3 minutes standing) each time. Use standing values if >80 years or if symptoms of postural hypotension are reported.
- If there is a 20-mmHg drop on standing, use erect BP for subsequent target and treatment decisions.
- For frail individuals, clinical judgement is encouraged prior to offering drug treatment.
- For stage 1 hypertension (clinic BP ranging from 140/90 mmHg to 159/99 mmHg), NICE recommends that we “discuss” drug treatment with adults aged <80 years.
- For grade 2 hypertension (clinic BP ranging from 160/100 mmHg to 180/120 mmHg), NICE gives much stronger advice to “offer” drug treatment.
- Use an ACE inhibitor or ARB as first-line treatment in all people living with diabetes, regardless of ethnic origin.
- When starting or changing diuretic treatment with a thiazide, it is now recommended to offer a thiazide-like diuretic (e.g. indapamide) in preference to a conventional thiazide such as bendroflumethiazide.
Resources
- At a glance: New NICE hypertension guidelines: http://bit.ly/2pL8Jgd
- NICE hypertension in adults:
www.nice.org.uk/guidance/ng136
Diabetes practice pearls
Kevin Fernando, GPwSI in Diabetes and Medical Education, North Berwick
- Consider an urgent, direct-access CT scan (within 2 weeks), or urgent ultrasound scan if CT not available, to assess for pancreatic cancer in people aged ≥60 years with weight loss and any of the following: diarrhoea, back pain, abdominal pain, nausea, vomiting, constipation and new-onset diabetes.
- HbA1c should be interpreted with caution in situations where red blood cell lifespan is affected (e.g. chronic iron-deficient anaemia or vitamin B12 deficiency) or where there is abnormal haemoglobin structure (e.g. HbS, HbF or sickle cell anaemia). Additional conditions, such as haemolysis, acute blood loss, haemodialysis, hypertriglyceridaemia, recent blood transfusion and venesection for haemochromatosis, can also invalidate HbA1c results.
- Features that point towards a diagnosis of maturity onset diabetes of the young (MODY) include: a strong family history of diabetes (any type) involving two or, ideally, three consecutive generations; onset from the second to fifth decade, usually <45 years; absence of features of insulin resistance; hyperglycaemia initially easy to control; and no history of diabetic ketoacidosis.
- Type 3c diabetes is diabetes of the exocrine pancreas, where structure and function of the pancreas is disrupted by disease (e.g. acute and chronic pancreatitis, cystic fibrosis, haemochromatosis and pancreatic cancer). Features that may point towards pancreatic exocrine insufficiency (PEI) include:
- Diarrhoea and steatorrhoea.
- Abdominal discomfort.
- Flatulence and bloating.
- Fatigue.
- Erratic blood glucose control if severe.
- Use a validated computer-based risk assessment tool to identify those at high risk of type 2 diabetes (e.g. QDiabetes-2018). QDiabetes-2018 predicts the absolute risk of developing type 2 diabetes over the next 10 years. 10% of the population has a >10% risk of developing type 2 diabetes over the next 10 years.
- Women with hypothyroidism require a 25–50% increase in thyroxine dose on conception. As a rule of thumb, increase levothyroxine by 25 mcg if the dose is <100 mcg, or by 50 mcg if the dose is >100 mcg.
- Reinforce sick-day guidance with SGLT2 inhibitors: temporarily stop the SADMAN drugs during any acute dehydrating illness and restart once eating and drinking normally (usually 24–48 hours later).
- SGLT2 inhibitors
- ACE inhibitors
- Diuretics
- Metformin
- ARBs
- NSAIDs
Resources
- Talking Head: Diabetes practice pearls:
http://bit.ly/2rF27Bd - GPnotebook Shortcut: Classification of diabetes: http://bit.ly/2PCyokp
- Diabetes Genes information on MODY: www.diabetesgenes.org
Dietary considerations in type 1 diabetes
Rose Butler, Diabetes Specialist Dietitian, Luton & Dunstable University Hospital
Carbohydrate counting in primary care
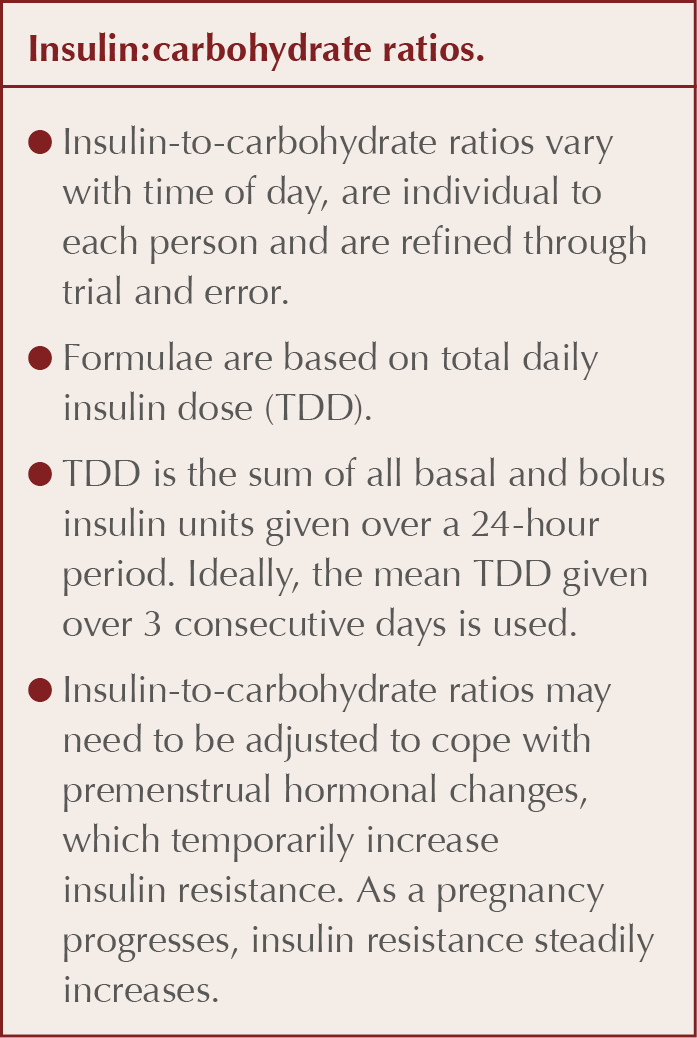
- The dietary focus for people living with type 1 diabetes is adjustment of rapid-acting insulin doses to match carbohydrate intake.
- Carbohydrate counting allows the individual freedom to eat what they want, when they want, while helping optimise glycaemic control.
- Offer referral to a diabetes specialist dietitian or to structured education courses, such as DAFNE or BERTIE. Signpost to web-based resources such as www.bertieonline.org.uk.
- The rate of carbohydrate digestion and degree of post-prandial blood glucose change is affected by the glycaemic index (GI) and glycaemic load (GL) of the carbohydrate, along with other macronutrients, such as fat or protein, that the carbohydrate is consumed with.
Supporting adults with type 1 diabetes to lose weight
- 60% of adults with type 1 diabetes in the UK are overweight or obese.
- The anabolic effects of insulin are greater when delivered exogenously. Weight loss requires a calorie deficit, which is challenging alongside managing glycaemia with insulin.
- Hypoglycaemia treatment is a major limiting factor that prevents weight loss. Treating a single hypo (with 15–20 g glucose + a small starchy snack) can add around 200 calories to the day’s intake.
- Hyperglycaemia can cause hunger and eating more than is needed.
Resources
- How to improve carbohydrate awareness:
http://bit.ly/2ztc4Ce
Practicalities of GLP-1 RAs and SGLT2 inhibitors
David Millar-Jones, GP with Special Interest and Associate Specialist in Diabetes, Cwmbran, and Nicola Milne, Community Diabetes Specialist Nurse, Manchester
- Guidelines are changing to encompass a more holistic approach to the care of people with type 2 diabetes, rather than purely focusing on glycaemic control.
- Some SGLT2 inhibitors and GLP-1 receptor agonists (RAs) have shown cardiovascular benefits. SGLT2is have also shown benefit in reducing renal disease progression and in heart failure.
- Healthcare professionals in primary care should be familiar with expected benefits and possible problems when prescribing these therapies.
- The prescriber should be familiar with each therapy’s mode of action. Any concerns around potential side effects and efficacy can be discussed fully with the patient and reassurance provided when necessary.
- GLP-1 RAs work by mimicking incretin hormones. Glucose lowering and weight loss are achieved through increased insulin and decreased glucagon secretion, and slowing of gastric emptying.
- This can result in gastrointestinal side effects and postprandial bloating.
- SGLT2is work by preventing glucose reabsorption in the kidneys and facilitating glucose excretion in the urine. As well as improving glycaemic control, they offer reductions in weight and blood pressure.
- Side effects include increased urine output and a risk of perineal and bladder infections.
- GLP-1 RAs are given as injections ranging from twice daily to once weekly (implants and oral therapies are in development). Each has a slightly different efficacy.
- The prescriber should be familiar with the different devices.
- SGLT2is are once-daily tablets, with similar efficacies.
- Medicine advisory agencies have stated that prescribers should inform patients about important side effects:
- GLP-1 RAs – risks of pancreatitis and a possible worsening of existing retinopathy.
- SGLT2is – risks of diabetic ketoacidosis, lower-limb amputation and Fournier’s gangrene.
- These risks have not been shown with all the therapies and in all the trials. Emphasis is placed on appropriate patient selection and counselling.
Resources
- Talking Heads: GLP-1 RAs and SGLT2is:
http://bit.ly/2Y5CwNw - PCDS Clinical Hub: GLP-1 RAs:
http://bit.ly/33Gegmq - How to use GLP-1 RA therapy safely and effectively:
http://bit.ly/2LVTRGx - How to use SGLT2 inhibitors safely:
http://bit.ly/2FbHdy9
Diabetes and pregnancy: Are we talking about the birds and bees?
Deborah Holder, Lead Diabetes Nurse, Thetford, and Nicola Milne, Community Diabetes Specialist Nurse, Manchester
Pre-conception
- There are higher levels of stillbirths, neonatal death and congenital abnormalities in women with pre-existing diabetes compared to the general population. This has not changed over 5 years.
- More women with type 2 diabetes are becoming pregnant than women with type 1 diabetes. These women are more likely to come from areas of social deprivation, which is an additional risk factor for adverse outcomes of pregnancy.
- Women with type 2 diabetes are likely to be managed solely by primary care prior to pregnancy. Give clear advice about the risks of being poorly prepared for pregnancy and offer support to achieve optimal pregnancy preparation.
- “Well prepared for pregnancy” means that prior to her last menstrual period, a woman has started 5 mg/day folic acid and stopped all adverse medication.
- Only one in eight women are well prepared for pregnancy. The proportions are similar for women with type 1 and type 2 diabetes, and have not changed since 2014.
Pre- and post-pregnancy advice
- Contraception: Encourage use when HbA1c is higher than desired, until a preferred level has been achieved.
- Folic acid: 5 mg/day prescription-only for 12 weeks prior to and 12 weeks after conception.
- Lifestyle: Women with a booking BMI ≥30 kg/m2 are at additional risk of adverse outcomes.
- Medication review: Stop ACE inhibitors, ARBs and statins. Metformin and insulin are the only antihyperglycaemic agents safe to use in pre-conception and pregnancy.
- Give capillary blood glucose targets:
- Fasting, 5–7 mmol/L.
- Pre-meal, 4–7 mmol/L.
- 2-hours post-prandial, <6.4 mmol/L.
- Ensure women have access to sufficient blood glucose monitoring equipment and refresh knowledge on hypoglycaemia for those taking insulin.
- For women with type 1 diabetes: Consider if flash glucose or continuous glucose monitoring is appropriate. Refresh patients’ knowledge on DKA and ensure access to ketone testing equipment.
- Monthly HbA1c test.
- Retinal screening: Pre- and during pregnancy.
- Renal review: Ensure that eGFR and microalbuminuria results are up to date.
- Smoking cessation: Advice as necessary.
- Specialist ante-natal services: Refer a woman with diabetes immediately once pregnant. She should be seen within 10 weeks of pregnancy.
Post-natal advice
- Breastfeeding can reduce the risk of progression to type 2 diabetes in women with gestational diabetes, and reduce risk of progression to type 2 diabetes in later life for baby.
- Ensure all women who have had gestational diabetes receive an annual review including HbA1c and ongoing lifestyle advice aiming to prevent progression to type 2 diabetes.
- Ensure appropriate management in any subsequent pregnancies.
Resources
- Talking Head: Preconception, contraception and gestational diabetes:
http://bit.ly/2syffIl - CPD: Pre-conception, pregnancy and postnatal advice to women with diabetes:
https://bit.ly/36XS2yt



Guest Editor Hannah Beba asks which outcomes – beyond mere numbers – are most important to the individual, the clinician and the NHS.
7 Jul 2026