

What and why: A new horizon for weight management in type 1 diabetes
● The prevalence of overweight and obesity has been increasing rapidly among people living with type 1 diabetes, challenging the historical perception of type 1 diabetes as a disease of lean individuals.
● This has led to the emergence of “double diabetes”, in which individuals with type 1 diabetes develop features typical of type 2 diabetes, including insulin resistance and metabolic syndrome.1
- Intensive insulin therapy, necessary for optimal glucose management, often drives further weight gain, creating a challenging clinical cycle.1–3
● Tirzepatide is a dual agonist of the glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors, which enhances satiety, reduces energy intake and improves glycaemic management.
- While currently licensed for type 2 diabetes and obesity management, use of tirzepatide in people with type 1 diabetes is rising due to its potential to address the cardiometabolic challenges of double diabetes.1,4,5
Tirzepatide licensing and funding context
Licensing: Although tirzepatide is not licensed for the treatment of type 1 diabetes, it can be prescribed to adults with type 1 diabetes when obesity is the primary indication, provided they meet the MHRA-approved criteria for weight management (BMI ≥30 kg/m2, or BMI 27–29.9 kg/m2 with at least one weight-related health problem).5
Funding: In view of the above, tirzepatide can, at least based on its licensing, only be obtained under the NHS through an obesity management service. In England, this would be uncommon as, at time of publishing, NHS England allows the medication to be prescribed in primary care under a funding variation6 for people with the following:
● Initial BMI ≥35 kg/m2 (as of June 2026) and at least four of the following long-term conditions:
- Hypertension
- Dyslipidaemia
- Established cardiovascular disease
- Obstructive sleep apnoea
- (Type 2 diabetes)
HSC obesity services are expected to commence in Northern Ireland in autumn 2026. Details are yet to be confirmed but there are likely to be strict criteria regarding BMI and other health conditions. Access in Wales is currently available through specialist Level 3 weight management services only, and tirzepatide is not yet available for obesity through any service in Scotland.
More commonly, people access tirzepatide through a private prescription.
Use in type 1 diabetes: Evidence and clinical rationale
While randomised controlled trials, such as SURPASS-T1D-1 (clinicaltrials.gov identifier NCT06914895) and SURPASS-T1D-2 (NCT06962280), are ongoing, growing real-world evidence suggests that tirzepatide may serve as an effective adjunct to insulin in people with obesity and type 1 diabetes.
● Substantial weight loss: Average weight loss ranging from 8.5% to 21.4% of total body weight, over 3–12 months.1,7–9 In a retrospective analysis, tirzepatide was associated with significantly greater weight loss than semaglutide (21.4% vs 9.1% reduction at 1 year).7
● Glycaemic improvement: Clinically meaningful HbA1c reductions ranging from 0.45% to 0.9%, with improved time in range and reduced glycaemic variability on continuous glucose monitoring (CGM).1,7–9
● Insulin dose reduction: Improvement in insulin sensitivity, leading to rapid and substantial reductions in total daily insulin requirements, often by 20–30% within the first 2–3 months.9,10
● Cardiometabolic benefits: Evidence suggests improvement in cardiometabolic risk factors, including blood pressure and lipid profiles.4
Safety considerations
Hypoglycaemia
● Tirzepatide slows gastric emptying. If a person administers their bolus (rapid-acting) insulin based on their usual “carb-counting” time (e.g. before or at the start of a meal), the insulin may peak before the glucose from the meal is absorbed.1
● This creates a mismatch, leading to post-prandial hypoglycaemia.
- Although proactive lowering of insulin doses may be useful in some people with tight glycaemic control, for most people the authors recommend that they adjust their insulin doses according to trends on CGM, especially post-prandial dips.
Diabetic ketoacidosis (DKA)
● While considered lower-risk than with SGLT2 inhibitors, DKA can still occur in people with type 1 diabetes taking tirzepatide, particularly if the insulin dose is reduced too aggressively or if the person becomes unwell (e.g. severe vomiting or diarrhoea, both of which are common side-effects of GLP-1-based treatments).10
● Author recommendations:
- Never stop basal insulin.
- Reduce prandial insulin only if necessary, and reduce gradually.
- Educate users on ketone testing and confirm availability of in-date testing equipment, even if glucose levels are normal.
Drug-related side-effects
● Nausea, diarrhoea or constipation, burping and reflux are common and usually transient.1,5,6
● There is a rare risk of developing pancreatitis and/or cholecystitis, occurring in approximately <3 in 1000 cases.5
● Consider gastroparesis in longstanding type 1 diabetes.
- Distinguish baseline symptoms from treatment-related effects by assessing for early satiety, post-prandial fullness, nausea, vomiting, abdominal bloating or unexplained glucose variability before starting therapy, and monitor for any worsening after initiation.
- Use slower titration or avoid use in those with significant symptoms.1,11
● Mitigate lean mass loss with ≥1.2 g/kg/day protein intake and resistance exercise.1
● Remain alert to disordered eating habits or body image disturbances, which could suggest a pre-existing eating disorder, or frequent insulin omission.1,12
Continuous glucose monitoring (CGM): A safety essential
Real-time CGM is fundamental to the safe use of tirzepatide in people with type 1 diabetes. As tirzepatide reduces insulin resistance and gastric emptying, CGM enables rapid insulin adjustments, early hypoglycaemia detection and close tracking of glycaemic variability.9,12
Key CGM targets
- Time in range (TIR): ≥70%
- Time below range (TBR): <4%
- Glycaemic variability: rising coefficient of variation suggests suboptimal glycaemic management and prompts review.
Practical use during tirzepatide therapy
A diabetes or weight management team should initiate tirzepatide. Dose escalation, insulin adjustments, CGM interpretation and any changes to automated insulin delivery (AID; e.g. hybrid closed-loop) settings should remain under specialist supervision.
Dose escalation: Review CGM data 1–2 weeks after each dose increase to reassess TIR, TBR and insulin needs. Increase the dose of tirzepatide by 2.5 mg every month until the target dose is reached. If the person is having side-effects, titrate the dose more slowly. Not all people will need to go to the maximum dose (15 mg weekly); many will see benefits even at the 5 mg weekly dose.
CGM alert settings: Set low-glucose alerts slightly higher than usual during initiation and escalation, to enable earlier correction.9
CGM sensor reliability: In cases of severe nausea, vomiting or dehydration, CGM readings may become unreliable, leading AID systems to overcorrect insulin delivery and raise DKA risk. In addition, when oral intake is low, a person may have a relatively normal glucose level yet display ketosis due to starvation from low carbohydrate intake.
- Confirm values with finger-prick blood glucose and check blood ketones even if CGM readings appear normal.1,12
AID systems: Data from adults with type 1 diabetes using semaglutide alongside hybrid closed-loop systems suggest that when insulin is proactively reduced and automated insulin delivery is in place, GLP-1-based therapy can improve weight and glycaemic metrics without increasing the risk of severe hypoglycaemia or DKA.13
- AID settings (insulin-to-carbohydrate ratios, correction factors and target glucose) may require adjustment during tirzepatide initiation and dose escalation, and temporary manual mode should be considered if CGM readings are unreliable.
The role of primary care
● Identify people with type 1 diabetes and obesity who may benefit from specialist assessment for weight management therapy.
● Ensure the person remains under ongoing specialist follow-up.
● Reinforce education on potential benefits (weight loss, lower insulin requirements) and risks (hypoglycaemia, ketosis/DKA).
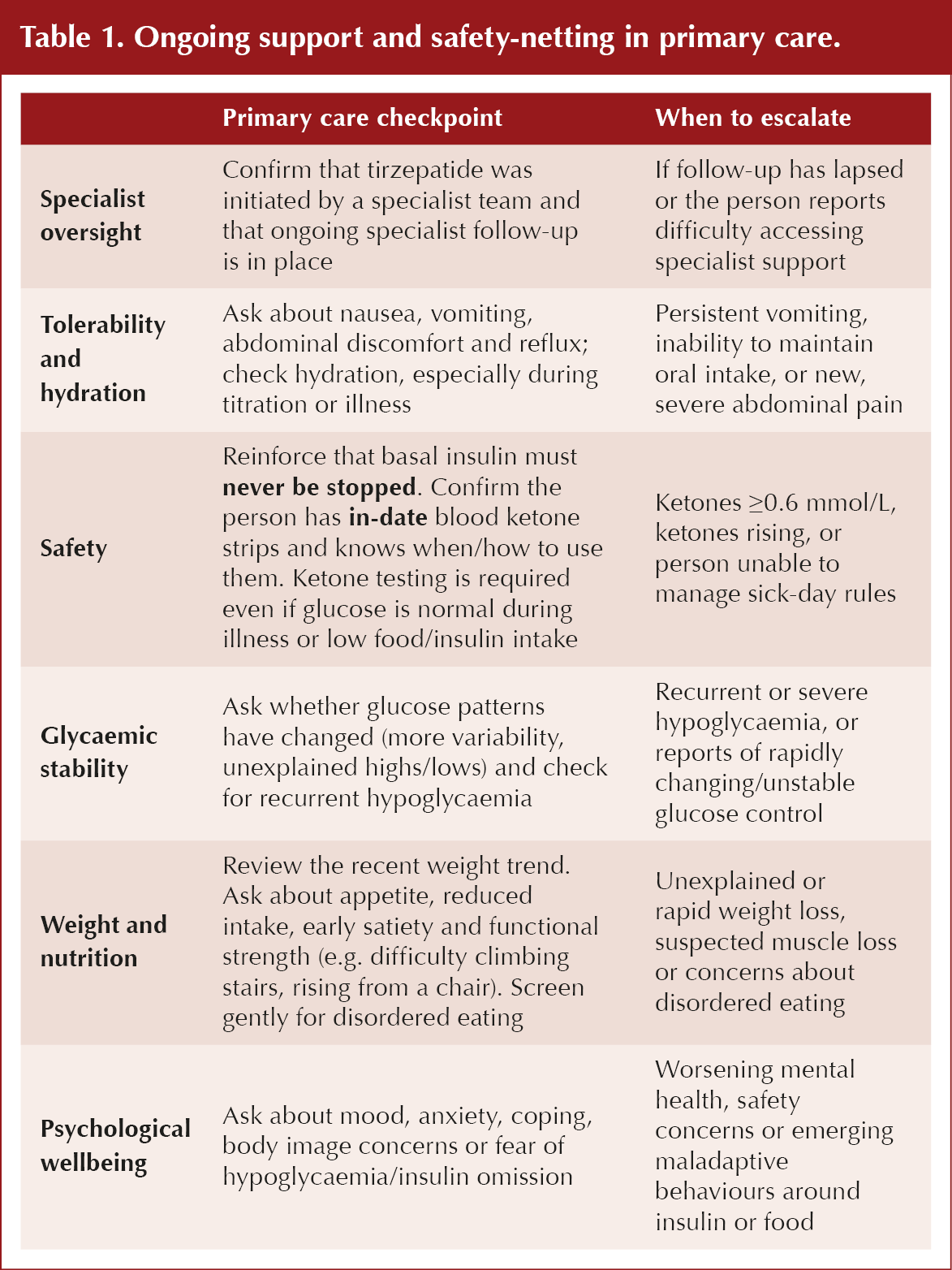
● Provide general monitoring and safety-netting once treatment has been initiated (e.g. review tolerability, hydration, sick-day understanding, weight trajectory). See Table 1 for more detail.
● Support holistic care, including blood pressure optimisation, cardiovascular risk management, psychological support and healthy living advice.
● Signpost promptly back to the specialist team if glycaemic control becomes unstable, if insulin requirements change rapidly or if adverse effects develop.
Note: Local policies vary, and some specialist services may not support continuation of incretin-based therapies in people with type 1 diabetes if initiated outside NHS pathways. Decisions regarding continuation or discontinuation should follow local governance and specialist team direction.
Summary
Tirzepatide is a promising adjunct for weight management in adults with type 1 diabetes and obesity, but its use requires individualised care and monitoring. Real-world studies support benefits in weight, insulin requirements, glucose variability and cardiometabolic risk factors; however, randomised controlled trials are needed to confirm these findings. Continuous glucose monitoring is essential, and primary care should reinforce education, monitor closely and refer early if safety concerns arise.
With shared-care models and proactive safety-netting, tirzepatide may help address a growing need in type 1 diabetes management.



Pragmatic guidance to help people optimise benefits from incretin-based weight loss drugs.
30 Jul 2026