

The Super Six model of diabetes care was implemented in September 2011 in Portsmouth Hospitals NHS Trust as a strategic response to the growing burden of diabetes management within acute and community settings (Kar, 2012; Nicholson et al, 2016). It was an innovative way for primary, community and specialist care to collaborate to meet the needs of people with diabetes and aim to improve their health outcomes. The model was founded on the principle that delivering optimal care does not require all individuals living with diabetes to be managed exclusively within hospital-based specialist services. Instead, it was recognised that, while certain aspects of diabetes care necessitated specialist oversight, much of routine management could be effectively delivered in primary care with appropriate support.
The Super Six model delineated six key clinical areas that would remain under the remit of specialist care (see Box 1). The model defined two core roles for consultants within specialist units: “specialist” and “educator” (Kar, 2012). The specialist role centred on leading the Super Six pathways within the Acute Trust, ensuring excellence in complex diabetes management and alignment with best practice guidelines. The educator role focused on supporting primary care in managing diabetes within the community, through both virtual and face-to-face engagement (see Box 2). The support was flexible and responsive to the needs of general practice teams. This collaborative structure evolved from the earlier Community Diabetes Team, established in 2007, which sought to improve diabetes outcomes through clinician education and patient self-management programmes.
Structural changes
Since the implementation of Super Six, the NHS Long Term Plan, first published in 2019, has introduced significant structural changes, including the move to Integrated Care Systems (ICSs), each led by an Integrated Care Board (ICB) and Integrated Care Partnership (NHS England, 2025). The neighbourhood care model, as mentioned in the Long Term Plan, further reinforces a shift towards care closer to home, community-based services and disease prevention, with hospitals reframed as community partners rather than solely acute providers. NHS Portsmouth CCG and South East Hampshire CCG were dissolved in 2022, with its responsibilities transferred to the Hampshire and Isle of Wight (HIOW) ICB.
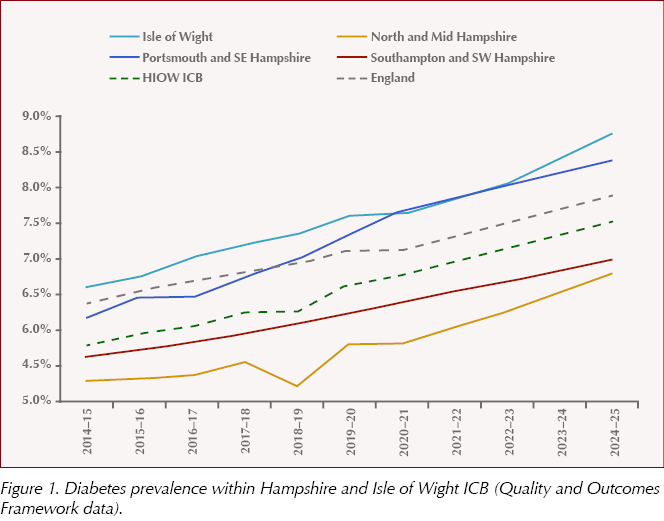
Within HIOW ICB, among a total population of around 2 million, diabetes prevalence has risen steadily from 5.8% in 2014/15 to 7.5% in 2024/25 (Figure 1). This represents an increase of 36,836 people on the diabetes register over the ten-year-period, equivalent to a 43% rise. The prevalence in Portsmouth and South East Hampshire is 8.4%, higher than both the HIOW ICB and England averages. It is also evident that the areas with highest diabetes prevalence align with the areas of greatest deprivation, with nine of the ten highest rates found in Portsmouth and South East Hampshire.
Outcomes after 5 years
The five-year evaluation of the Super Six model, conducted in 2016, demonstrated measurable improvements in clinical outcomes, reductions in diabetes-related hospital admissions and vascular events, and associated cost savings for the NHS (Nicholson et al, 2016). The review also reported high levels of satisfaction among both patients and primary care practices. Additional benefits included enabling the specialist team to dedicate greater focus to engagement and education for young people with type 1 diabetes, strengthening inpatient foot care provision and fostering collaborative research initiatives.
Outcomes after 15 years
In this article, we review the clinical outcomes again, 15 years after implementation. Outcome measures included diabetes-related hospital admissions; long-term vascular events; and compliance with treatment targets and eight care processes based on the National Diabetes Audit.
Hospital admissions where diabetes was recorded as the primary diagnosis have risen overall by 35.7% within HIOW ICB, although the rate of increase varies across providers. Notably, Portsmouth Hospitals University NHS Trust (PHU) has experienced the lowest rise in admissions, at 26.2%.
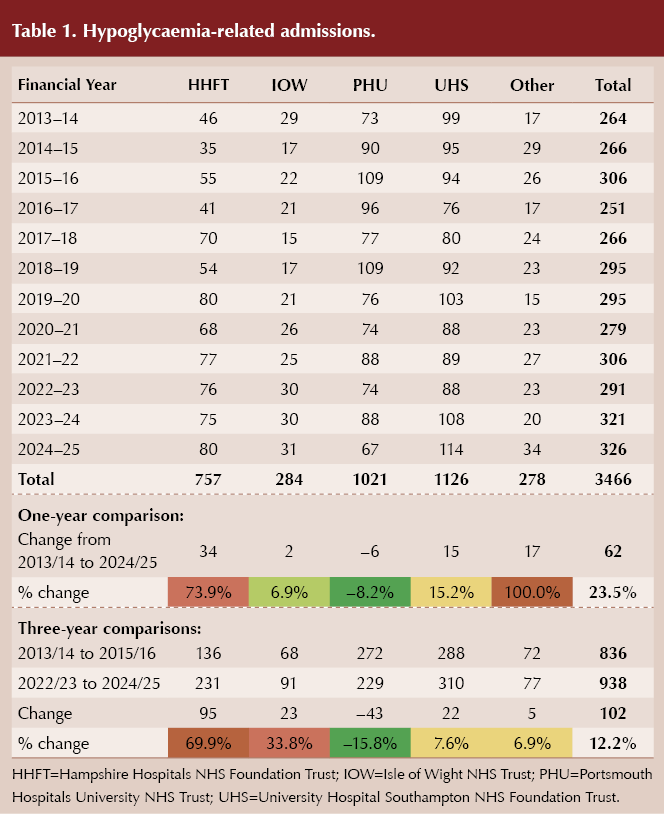
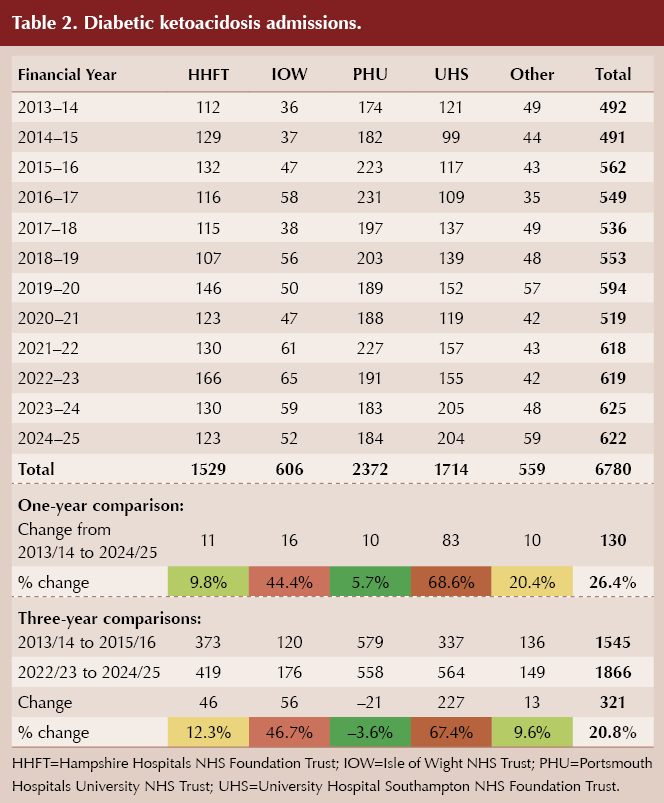
When comparing the three-year periods of 2013/14–2015/16 and 2022/23–2024/25, PHU shows a 15.8% reduction in hypoglycaemia-related admissions and a 3.6% reduction in diabetic ketoacidosis admissions (Table 1 and Table 2).
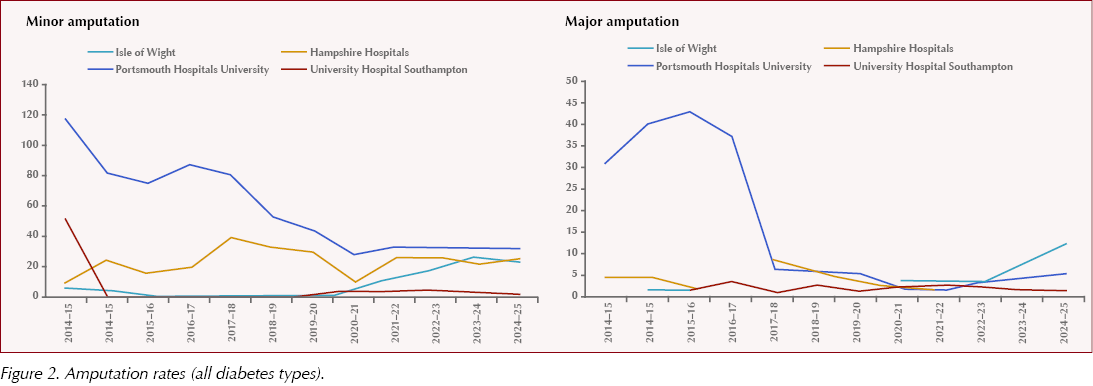
Over the same decade at PHU, both minor and major amputation rates among people with diabetes have continued to decline significantly (Figure 2). This has been made possible with the provision of multidisciplinary foot clinics and joint vascular foot clinics, as well as inpatient podiatry services.
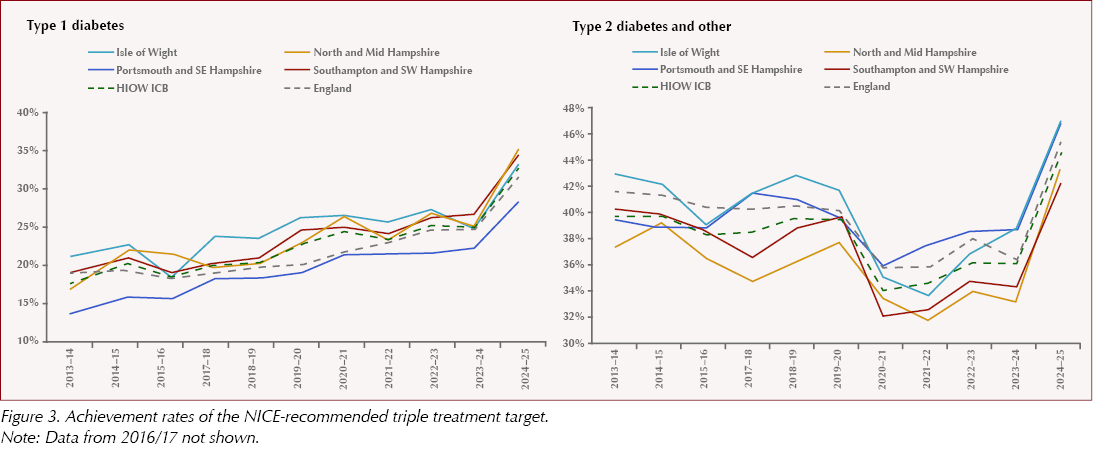
In terms of meeting the three treatment targets recommended by NICE (HbA1c ≤58 mmol/mol, blood pressure ≤140/80 mmHg and prescription of a statin), there has been continuous improvement within the last decade for both type 1 and type 2 diabetes, except during the COVID-19 pandemic, and there was a sharp increase last year (Figure 3).
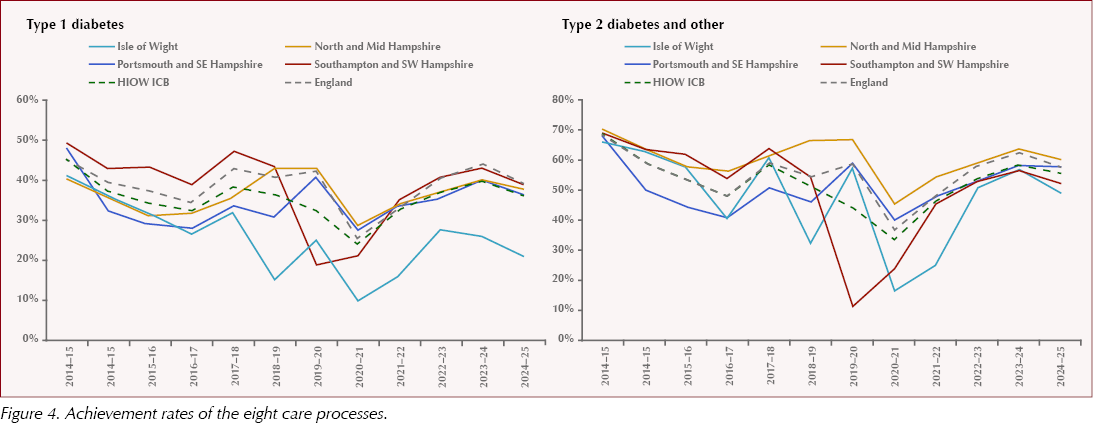
The percentage of people with type 1 and type 2 diabetes meeting all eight care processes in Portsmouth and South East Hampshire is below the England average, and was affected during the COVID-19 pandemic between 2020/21. Over the course of the decade, the proportion of individuals receiving all eight care processes has reduced (Figure 4). This might be attributed to a number of factors, including challenge to access with increased rates of deprivation, inconsistencies in diabetes care, workload pressures on the general practice workforce, and others.
There has been an increase in referrals to secondary diabetes specialist services since the introduction of the NICE (2023) TA943 Technology Appraisal, which recommends hybrid closed-loop (HCL) systems for managing blood glucose levels in adults with type 1 diabetes who have an HbA1c of 58 mmol/mol or higher, experience disabling hypoglycaemia, or are planning a pregnancy or currently pregnant. As the 5-year phased roll-out of HCL progresses, demand for access to the technology continues to grow, and the Super Six Model supports timely assessment and management of these referrals. This has been offset by reductions in referrals to foot and renal clinics, due to the focus on prevention work in the community.
Conclusions
Fifteen years on, the Super Six model continues to demonstrate both positive clinical impact and system-wide value. While it is not a complete solution, the latest review of outcomes, together with National Diabetes Audit data, has shown sustained improvements across many key measures.
Interpretation of these results requires caution due to several confounding factors, including changes in care models (e.g. same-day emergency care), the COVID-19 pandemic and variations in hospital coding, which mean that long-term comparisons may not be directly equivalent. Taken collectively, however, these findings provide strong evidence that the model remains effective despite substantial growth in diabetes prevalence, rising complexity and the wider operational pressures facing the NHS over the past decade.
A main contributor to this continued success is the unique structure of the Super Six model itself. Unlike other local approaches that separate acute and community diabetes care across different teams or providers, the Super Six model embeds one cohesive specialist team across both hospital and community settings. This continuity enables quicker decision-making, consistent clinical standards and seamless escalation or de-escalation of care. It also ensures that primary care receives timely, reliable guidance from the same specialists who manage the most complex cases, maintaining confidence and shared accountability.
This model and collaborative approach has become increasingly relevant within the context of new NHS vision and structure, rising diabetes prevalence and increasing demand for advanced therapies such as HCL technology. As care pathways become more complex, the ability to have a single specialist team overseeing acute, community and educational functions has proven to be a fundamental differentiator. It offers improved outcomes, more efficient use of resources and a model of partnership that remains highly valued by both patients and primary care in managing diabetes as a chronic condition.


High intake of ultra-processed foods associated with cardiovascular morbidity and mortality. How can we mitigate this risk?
25 Jun 2026