

| Case presentation |
| Mrs Ryan is a 74-year-old lady with a background of type 2 diabetes, hypertension, hyperlipidaemia and a previous transient ischaemic attack. Her medication list includes: • Metformin. • Atorvastatin. • Ramipril. • Clopidogrel. • Amlodipine. • Furosemide. • Solifenacin. She is attending today for her routine diabetes appointment, and you are reviewing her medication, noting her expressed concerns that she feels she is taking “too many tablets” and finds it “hard to remember to take them.” You go through the timeline of her medication additions and notice an interesting pattern emerge. Just over a year ago, Mrs Ryan developed ankle swelling. She was seen in the practice and requested furosemide for this, as her sister used it for her ankle swelling and found it very helpful. The prescription was only supposed to be a short-term medication, pending an echocardiogram that did not happen. However, it became a regular medication without further thought; Mrs Ryan was content with this, given her sister’s vouching for the diuretic. Subsequently, she began experiencing urinary urgency and frequency, which was attributed to an overactive bladder, and solifenacin was added to her regimen. Mrs Ryan now worries that a recent reduction in her memory is making the management of a complex medication regimen difficult. As you hear her medication history narrated so succinctly, you note the addition of amlodipine to her regimen a month prior to her initial presentation with ankle swelling. It occurs to you that Mrs Ryan may have fallen foul of a “prescribing cascade”. |
Polypharmacy represents a considerable challenge for older adults with type 2 diabetes and those living with multimorbidity (Hickman et al, 2023). Polypharmacy can elevate the risk of adverse drug events and falls, and may not always align with patient preferences (NICE, 2016; Dhalwani et al, 2017). It is essential, therefore, to practise pharmacovigilance in people with type 2 diabetes who are experiencing adverse reactions from polypharmacy, and to evaluate the benefits of each medication to identify those that may be non-beneficial or inappropriate. Among people with multiple chronic conditions or difficulties adhering to complex medication regimens, conducting a comprehensive medication review can be particularly valuable.
What is a prescribing cascade?
Prescribing cascades arise when adverse drug reactions or side effects of an initial medication or index drug are managed by introducing additional medications (Shahid et al, 2024; Nielen et al, 2025). The concept has been recognised for over two decades (Chen et al, 2023), but research regarding the many different prescribing cascades is ongoing (Shahid et al, 2024).
While certain prescribing cascades may be intentional and clinically appropriate – such as the initiation of a proton pump inhibitor to reduce gastrointestinal bleeding risk in people on direct oral anticoagulants with other risk factors for bleeding – a fundamental issue driving inappropriate prescribing cascades is the misinterpretation of medication side effects as entirely new medical conditions (Tejani and Perry, 2025). In fact, many cascades are inadvertent, inappropriate and potentially detrimental (McCarthy et al, 2019), as we suspect in the case of Mrs Ryan.
Contribution to polypharmacy: A global concern
Unfortunately, prescribing cascades exacerbate the prevalence of polypharmacy and its associated risks (Tejani and Perry, 2025). Globally, addressing the burden of polypharmacy and reducing medication-related harms remain the central aims of various initiatives, including the Medication Without Harm campaign (World Health Organization, 2024).
Vulnerable groups
Evidence indicates that older adults from lower socioeconomic status (defined by income or education) experience higher rates of polypharmacy and coprescribing – often indicative of prescribing cascades – compared to those with higher socioeconomic status (Rochon et al, 2025). Within lower socioeconomic groups, women are disproportionately affected by coprescribing relative to men.
Common prescribing cascades
This topic would be much more simple for us in primary care if there was a small list of prescribing cascades. However, this issue is complex and evolving. The literature has identified 94 potential prescribing cascades to date, with varying levels of supporting evidence. In a recent review, Shahid et al (2024) grouped these prescribing cascades into four categories, with level 1 representing the cascades with the most supporting evidence. Table 1 summarises these level 1 prescribing cascades.
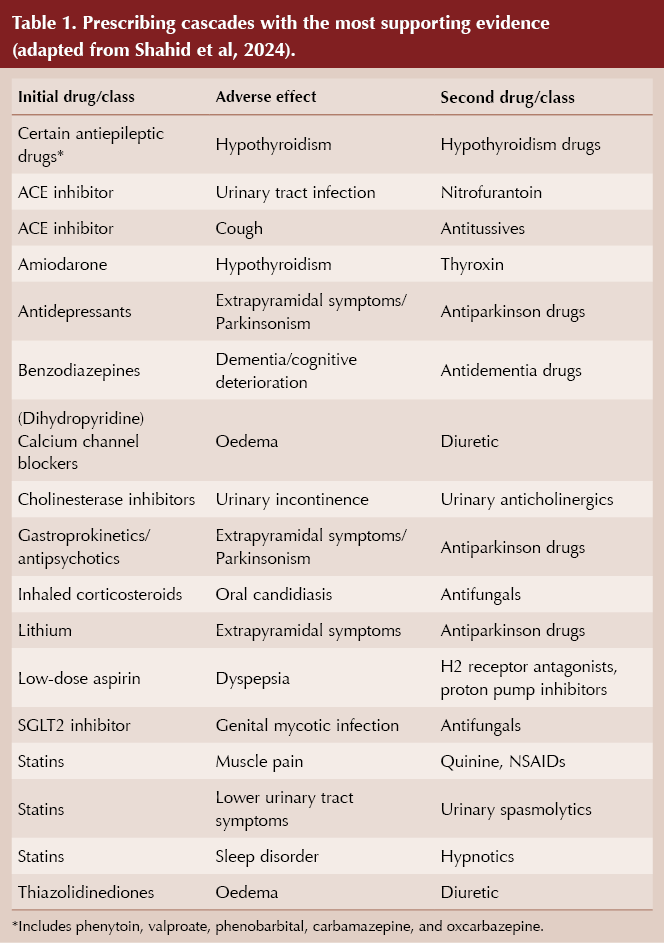
Medications commonly taken by people living with type 2 diabetes feature strongly in this list. Notably, there is level 1 evidence to support a prescribing cascade in which SGLT2 inhibitors cause genital mycotic infection, requiring subsequent prescription of antifungals. Antihypertensives, which are also commonly prescribed in people living with type 2 diabetes, feature as well, with calcium channel blockers resulting in oedema and subsequent prescription of diuretics, and ACE inhibitors causing cough, warranting the prescription of antitussive medications.
Statins, also very commonly prescribed in type 2 diabetes, feature in multiple prescribing cascades, as their side effects include muscle pain (leading to prescription of NSAIDs or quinine), lower urinary tract symptoms (leading to prescription of urinary antispasmodics) and sleep disturbance (leading to prescription of hypnotics).
Other research indicates that the most common prescribing cascade involves the use of diuretics to treat oedema caused by calcium channel blockers, while the second most frequent is bladder anticholinergics to treat incontinence caused by cholinesterase inhibitors (Trenaman et al, 2021).
Taking action against prescribing cascades
Deprescribing is a structured approach used in clinical practice to safely reduce medications by simplifying regimens, lowering doses or completely discontinuing them to help prevent or address polypharmacy (Jude et al, 2022). Numerous studies have shown that polypharmacy is increasingly common among people with type 2 diabetes, which underscores the value of deprescribing within effective prescribing practices.
There are four main deprescribing strategies (Aubert et al, 2021):
1. Entirely stopping a medication.
2. Gradually lowering the dosage.
3. Reducing the medication dose.
4. Switching to a different medication with a more favourable risk–benefit profile.
While further evidence on prescribing cascades is needed, the NICE NG56 guideline on multimorbidity reminds us to consider the benefits versus the harms of medications and the burden of treatment, and to consider deprescribing where appropriate (NICE, 2016).
| Mrs Ryan’s case conclusion |
| When we last left Mrs Ryan’s case, you were suspicious that her medication list may have included some inappropriate prescribing cascades. Based on the timeline Mrs Ryan has outlined to you, it is likely that you are correct and the following events have occurred. Amlodipine was initiated for Mrs Ryan’s hypertension. This resulted in peripheral oedema. Unfortunately, this was not recognised as a side effect of her calcium channel blocker and she was placed on furosemide to treat this for a short time, which became longer-term due to a change in healthcare practitioner. A second prescribing cascade occurred when the furosemide increased her urinary frequency. Again, this was interpreted as a new medical condition of overactive bladder, as opposed to a medication side effect, resulting in a prescription for solifenacin. Solifenacin is known to cause cognitive side effects in older adults, and this has caused the memory impairment which prompted Mrs Ryan to ask for simplification of her medication regimen today. Thankfully, it is now possible to slowly retrace Mrs Ryan’s steps and systematically deprescribe the offending medications involved in these prescribing cascades. This resulted in a much shorter medication list for Mrs Ryan, with the elimination of solifenacin, furosemide and amlodipine. Once her amlodipine was stopped, her ramipril was uptitrated to control her blood pressure. This resulted in the resolution of all of her medication side effects, and a great deal of satisfaction on both her and your part. Key learning outcomes Awareness of the presence of common prescribing cascades, their contribution to polypharmacy, risk of adverse drug reactions and increased patient burdens, especially in vulnerable groups, is important for us in primary care. Avoiding and addressing prescribing cascades can have positive effects on people living with type 2 diabetes, other chronic conditions, polypharmacy and multimorbidity. |
Useful resource
At a glance factsheet: Deprescribing in type 2 diabetes. Diabetes & Primary Care 25: 77–8. Available at: https://diabetesonthenet.com/diabetes-primary-care/factsheet-deprescribing/


High intake of ultra-processed foods associated with cardiovascular morbidity and mortality. How can we mitigate this risk?
25 Jun 2026