

Antiplatelet agents for primary prevention of cardiovascular disease
● Avoid routinely using antiplatelet agents for primary prevention of cardiovascular disease.1,2
- This advice extends to people with diabetes – do not routinely offer antiplatelet therapy to people with type 1 or type 2 diabetes in the absence of cardiovascular disease.3,4
● In people at very high risk of myocardial infarction or stroke, antiplatelet agents may be offered if benefits outweigh risks in an individual case.1 Thus, low-dose aspirin may be considered for primary prevention in people with diabetes with a high degree of cardiovascular risk who are not at increased risk of bleeding.5
Although low-dose aspirin does result in a small reduction in risk of serious cardiovascular events (relative reduction 12%), this was negated by a 30% higher incidence of bleeding, principally gastrointestinal.6
Antiplatelet agents for secondary prevention of cardiovascular disease1
Antiplatelet agents offer clear benefits for cardiovascular protection in those with established atherosclerotic cardiovascular disease – i.e. for secondary prevention.6
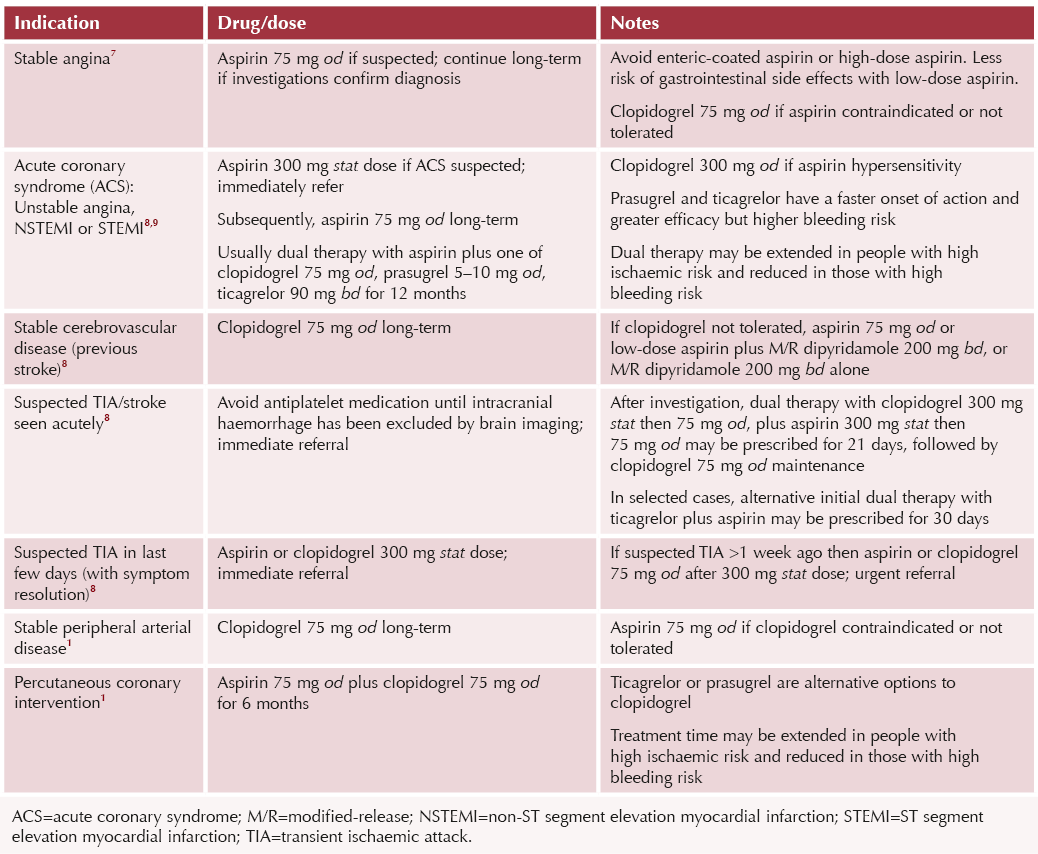
● Other than an immediate loading dose of antiplatelet therapy for acute coronary syndrome (ACS), treatment will usually be initiated by hospital specialists for ACS, stroke/transient ischaemic attack or percutaneous coronary intervention.
● For stable cardiovascular disease and/or peripheral vascular disease, the combination of aspirin with low-dose rivaroxaban (i.e. antiplatelet plus anticoagulant therapy) may bring added benefits for secondary prevention, and can be considered in those at low bleeding risk.1,5
● Anticoagulant agents rather than antiplatelet agents are recommended for management of atrial fibrillation.
Recommended indications for antiplatelet agents for secondary cardiovascular prevention
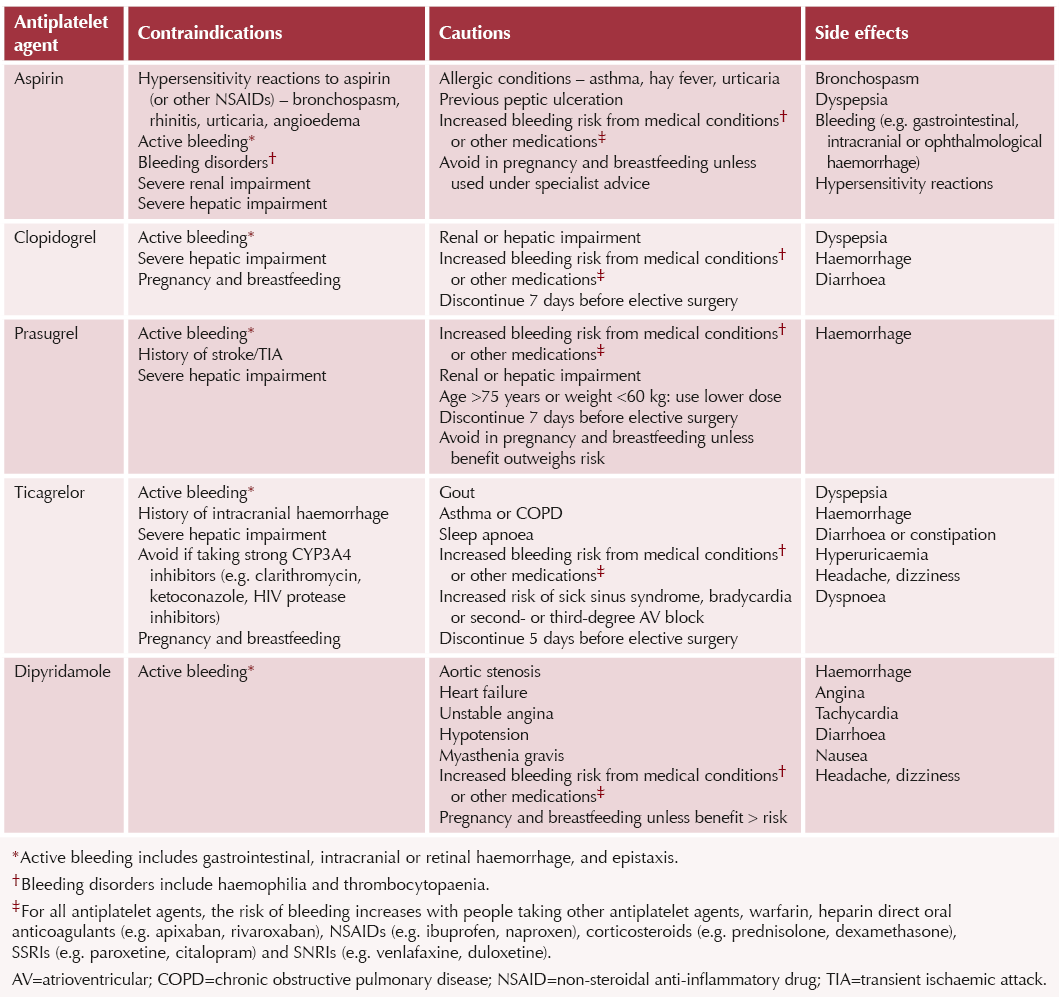
Contraindications, cautions and side effects of antiplatelet agents
Antiplatelet drugs and dyspepsia1
Dyspepsia describes upper gastrointestinal (GI) symptoms including upper abdominal pain, acid reflux, nausea and vomiting. It is a common side effect of antiplatelet agents.
People at high risk of GI side-effects:
- Older age, especially >75 years.
- History of gastroduodenal ulceration/perforation or GI bleeding.
- Helicobacter pylori infection.
- Concomitant use of other agents that predispose to GI bleeding: additional antiplatelet medication, warfarin, heparin, DOACs, NSAIDs, corticosteroids, SSRIs, SNRIs.
Managing people taking antiplatelet medication at high risk of GI side-effects
● Add proton pump inhibitor (PPI) for gastroprotection.
- Avoid omeprazole and esomeprazole when using clopidogrel, as they can lead to reduced plasma levels of activated clopidogrel. Other PPIs can be used.
● A histamine H2 antagonist (e.g. famotidine) can be used if PPIs are contraindicated or poorly tolerated.
Treating antiplatelet-induced dyspepsia
● If alarm features (e.g. dysphagia, weight loss, jaundice), refer urgently. Refer immediately if active GI bleeding.
● If no alarm features, consider antacid or alginate for symptom relief on an as‑required basis.
● Offer PPI for 1 month. Test and treat for H. pylori (a 2-week delay after finishing a PPI is required before testing).
- Use alternative PPI to omeprazole and esomeprazole if taking clopidogrel.
● Use H2 antagonist if PPIs are contraindicated or poorly tolerated.
● If symptoms recur after initial PPI treatment or H. pylori elimination, use maintenance PPI at lowest dose to control symptoms.
● If symptoms persist despite treatment, refer for investigation.



Pragmatic guidance to help people optimise benefits from incretin-based weight loss drugs.
30 Jul 2026