

| Key learning points |
| • With an ageing population, the incidence of both dementia and diabetes is rising and the co-morbidity of these two conditions is increasingly common. This has pro-found personal and social consequences. • People with diabetes have an increased risk of cognitive decline and dementia. Type 2 diabetes is associated with a 2.5-fold increased risk of vascular dementia and a 1.5-fold increased risk of Alzheimer’s disease. • Both hyperglycaemia and medication-induced hypoglycaemia are responsible for cognitive decline in people with diabetes. • People with dementia are likely to have difficulty managing their diabetes, including making healthy lifestyle choices, adhering correctly to medication regimens and monitoring blood glucose levels. |
The nature and prevalence of dementia
● Dementia is a condition characterised by cognitive impairment to the degree that it compromises the ability to lead a normal life. It is typically a progressive, irreversible condition.
● Many areas of cognition can be adversely affected, including memory, attention and concentration; language; planning and organisation; problem solving and decision making; and social skills.2
● By the end of 2025, it is estimated that 1 million people in the UK will have a diagnosis of dementia, and this number is forecast to double over the next 20 years.3
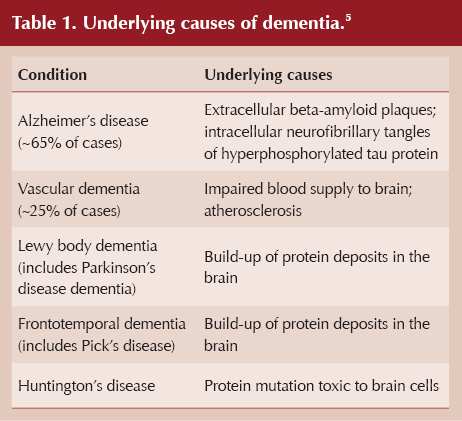
● The presentation of dementia will depend on the sub-type. Alzheimer’s disease is the most common form of dementia, followed by vascular dementia (Table 1). Other forms of dementia are Lewy body dementia and frontotemporal dementia.4
Diabetes as a risk factor for dementia
● Diabetes is associated with an increased risk of cognitive impairment and dementia.
- People with type 2 diabetes have a 1.5–2.0-times greater incidence of all-cause dementia compared to the population without diabetes.6
- Cognitive decline in older adults with type 2 diabetes proceeds at twice the rate of those without diabetes.7
- A recent US study found the prevalence of dementia in adults with diabetes to be 13.1% in 65–74-year-olds and 24.2% in the over-75s.6
● The subtypes of dementia most strongly associated with type 2 diabetes are vascular dementia (2.5-fold increased risk compared to no diabetes) and Alzheimer’s disease (1.5-fold increased risk).8
● Type 1 diabetes is also linked to a higher incidence of dementia, notably when extremes of glycaemia (low or high) have been experienced.9
● In the ACCORD-MIND trial in people with type 2 diabetes, higher HbA1c levels were associated with lower cognitive function.10 Further studies, such as AgeCoDe, have confirmed this link.11
- However, the extension of the ACCORD-MIND trial showed that intensive glycaemic intervention did not result in improved cognitive outcomes.12
How does diabetes contribute to cognitive decline?
● Atherosclerotic disease of cerebral arteries contributes to cognitive decline; this pathology is more pronounced in people with diabetes.
● Vascular dementia is a relatively more common cause of dementia in people with diabetes compared to the population without diabetes.
● Chronic hyperglycaemia generates advanced glycation end-products (AGEs), with glucose covalently bonding to proteins and other important molecules, thereby damaging their function.13 Microvascular damage results, with accompanying inflammatory changes including acceleration of amyloid plaque formation (affecting Alzheimer’s disease).
● Insulin receptors are present in the brain, notably in the cerebral cortex and the hippocampus, which is central to memory function. In people with diabetes, insulin resistance at this local level will compromise glucose utilisation, drive inflammatory change and damage neuronal function.14
● Neuronal damage can also arise in response to acute hyperglycaemia. In this situation, there can be a reduction in cerebral blood flow that exposes cells to oxidative stress and subsequent molecular damage within cells.9
Hypoglycaemia and dementia
● There is mounting evidence that episodes of hypoglycaemia lead to cognitive decline and increase the risk of dementia. The more frequent and severe these episodes, the greater the risk.9
● Sulfonylureas, meglitinides and insulin are the treatments most likely to induce hypoglycaemia.
● Intensive insulin therapy, most commonly in the context of type 1 diabetes, carries the highest risk of hypoglycaemia.15
● Dementia itself increases risk of hypoglycaemia for multiple reasons (see Table 2).1,16 The ensuing neuroglycopenia can lead to permanent neuronal damage.9
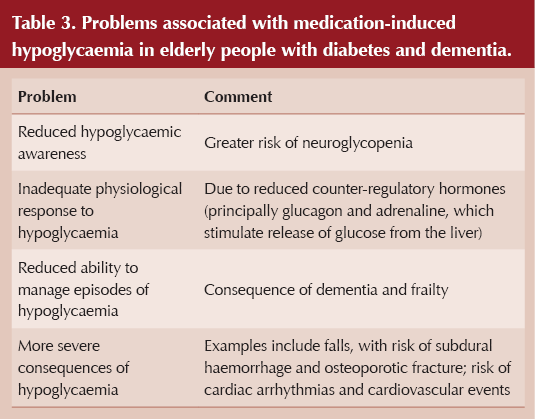
● People with dementia, and elderly people in general, are at greater risk of medication-induced hypoglycaemia and of more serious consequences from this – see Table 3.

Depression, diabetes and dementia
● Depression is a risk factor for dementia.
● People with type 2 diabetes are more prone to depression than those without diabetes.6
● Individuals with diabetes who suffer from depression are 2.7-times more likely to develop dementia than those with diabetes alone.17
Consequences of dementia for managing diabetes
● Education and empowerment of an individual to self-manage their diabetes is compromised with the co-morbidity of dementia.18
● People with dementia may lack the ability to make healthy lifestyle choices that are important in managing their diabetes, notably diet and exercise.19
● Medications may be taken incorrectly or not at all.
- In the case of antidiabetes medications, this places the individual at risk of both hyper- and hypoglycaemia, both of which can accelerate cognitive decline.16
- Missing treatments for hypertension and dyslipidaemia increases the risk of cardiovascular complications.
● Self-monitoring of blood glucose levels may not be possible, so that persistent hyperglycaemia or episodes of hypoglycaemia pass unidentified.
● In addition to problems with memory, organisation and planning, people with dementia may be further burdened with behavioural and psychological symptoms that compromise diabetes management.20
Useful resources
● How to manage diabetes in later life
● How to prevent, identify and manage hypoglycaemia in adults with diabetes
● At a glance factsheet: Deprescribing in type 2 diabetes
● Diabetes Distilled: The 4S Pathway – realigning management for older people with diabetes




ICBs in England are undergoing a major restructure. Guest editor Hannah Beba asks how this might affect diabetes care.
9 Jul 2025