

Prevalence and overview
Female sexual dysfunction (FSD) encompasses persistent, recurrent problems with sexual arousal, desire, orgasm and or pain that causes distress. Sexual dysfunction in women with living with diabetes is approximately twice as common as in women without diabetes. A recent meta-analysis and systematic review reported an overall prevalence of 58.81% among women with diabetes, with those who are living type 2 diabetes being particularly affected, showing a prevalence of 71.03% (Gebeyehu et al, 2023).
Contributing factors
- Low or high glucose levels may result in:
- Lack of vaginal lubrication.
- Pain during sexual activity.
- Structural changes in female genital tissue plus impairment of nerve and blood supply, which might impact on the arousal and orgasmic sexual response.
- Higher rates of depression and diabetes-related distress (e.g. diabetes-related burnout) can lead to low sexual drive.
- Affecting 10% of adult females with or without diabetes, hypoactive sexual desire disorder (HSDD) is associated with negative emotional and psychological states, and medical conditions including depression.
- Depressive symptoms are independently and bidirectionally associated with HSDD, with the presence of depression conferring a 50% to 70% increased risk of sexual dysfunction, and the occurrence of sexual dysfunction being associated with a 130% to 210% increased risk of depression (Clayton et al, 2018).
- Adding a layer of complexity, most antidepressants are associated with decreased sexual desire.
- Wearing of diabetes devices, such as insulin pumps and continuous glucose monitors, may affect body image and self-esteem.
- Skin changes from lipohypertrophy around insulin injection sites may also affect body image and self-esteem.
- The burden of self-managing diabetes may affect the spontaneity of sex (Winkley et al, 2021).
Perimenopause and menopause can affect sexual well-being even in the absence of diabetes; however, women with diabetes may experience these effects more severely (Vallibhakara et al, 2026).
Clinical impact and importance of recognition
Untreated sexual dysfunction can lead to relationship difficulties and breakdown. In addition to being a quality-of-life concern, FSD frequently stems from the same underlying physiological damage that contributes to heart disease and nerve damage throughout the body. Women with FSD may, therefore, be at increased risk of developing cardiovascular and neurological complications (Navriya et al, 2025).
Research into female physiology, sexual function and sexual response remains limited in comparison to male sexual health, and requires further development to support evidence-based assessment and treatment options for women. Improving women’s understanding of normal female sexual physiology and the changes associated with sexual arousal may also support earlier recognition and discussion of sexual dysfunction. For healthcare professionals (HCPs), it is important to recognise that sexual well-being is highly individualised, and that sexual activity or intimacy may not be a priority for all women, including those who identify as asexual.
Raising awareness of the problem may help women living with diabetes and HCPs to discuss it as part of routine diabetes clinical consultations.
Communication and barriers to discussion
It is reported that:
- 72% of women with female sexual dysfunction would like to talk to their HCP about their difficulties.
- 73% of these women would like their HCP to initiate the conversation (Kingsberg et al, 2019).
Possible barriers for healthcare professionals
- Time constraints, including time-limited appointments.
- Not part of “core services”, not funded or not measured (e.g. QOF).
- Lack of confidence – we do not feel that we have the right skills to open a conversation about sexual health and diabetes.
- We do not know how to provide support or have availability and to access additional support/services.
- Lack of availability, limited access and long waiting times for sexual health services.
- We assume the person would not want to be asked such personal questions.
- We are reluctant to “open a can of worms”.
- Perception that female sexual dysfunction is to be expected because of the “ageing” process.
- We may not think it is important.
Women’s sexual health needs and perspectives may vary according to cultural and environmental factors; therefore, HCPs should approach discussions around sexual dysfunction with sensitivity and cultural awareness.
Assessment and screening tools
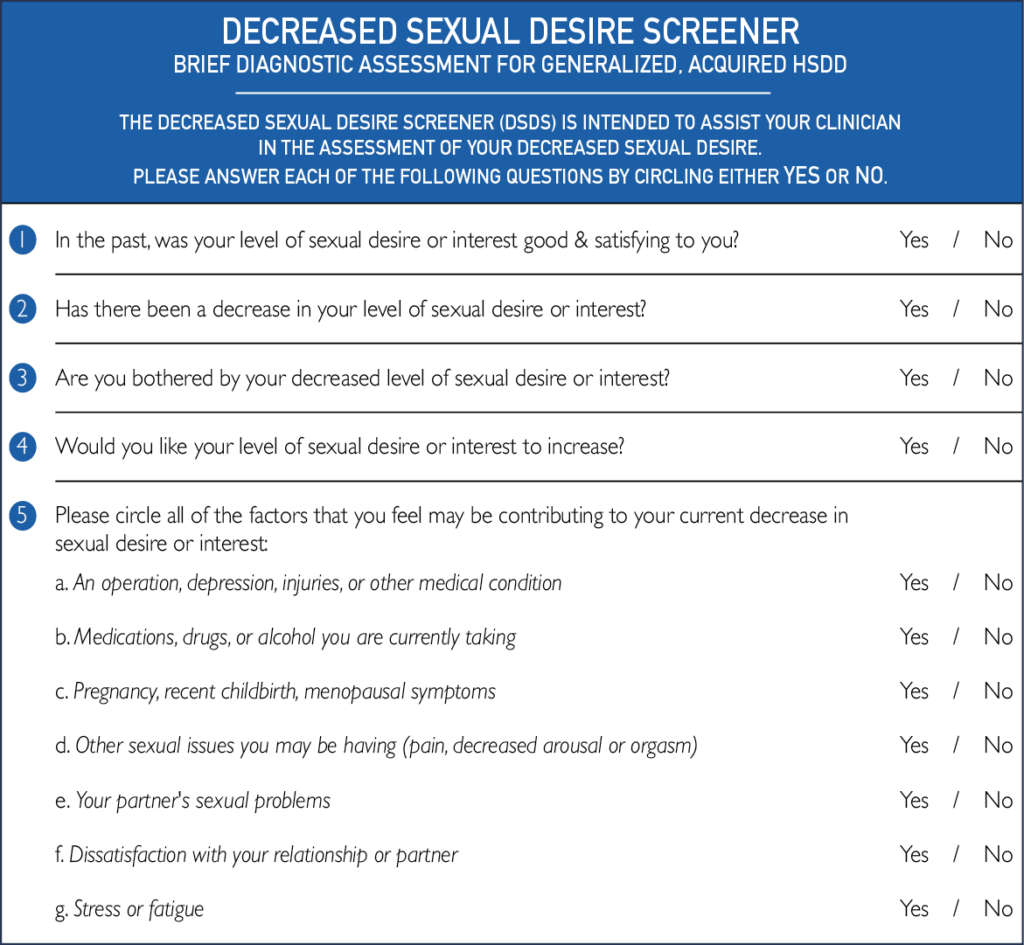
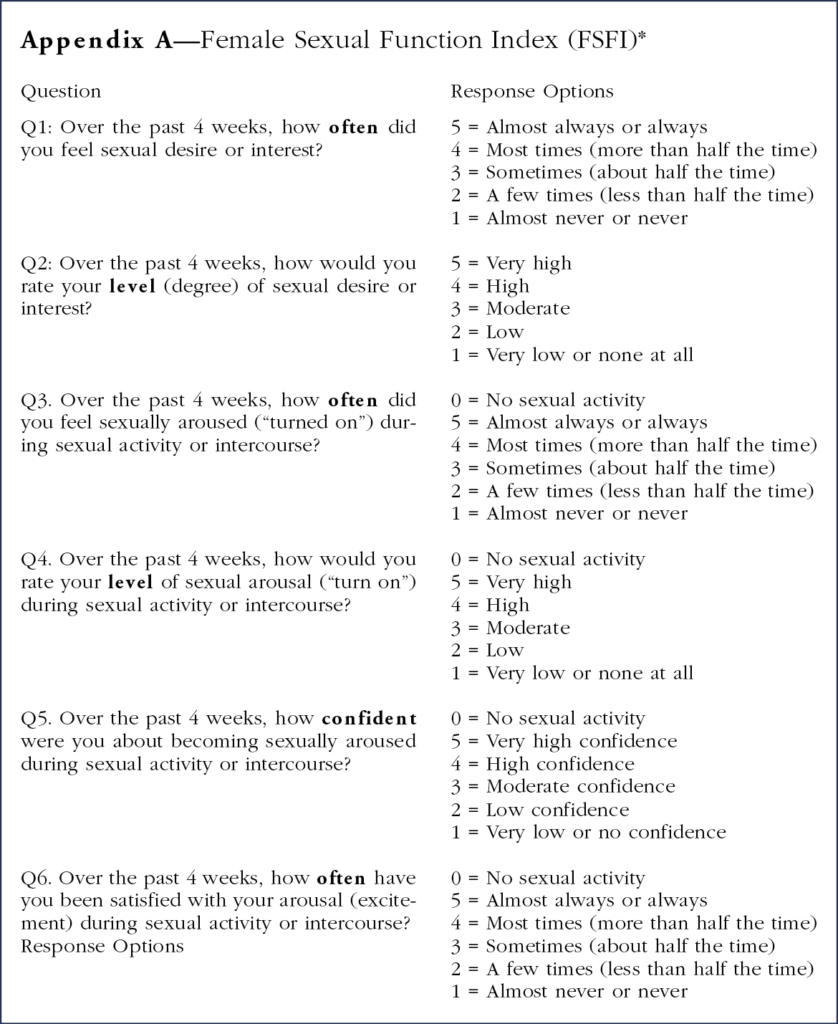
Self-report questionnaires or clinician checklists may assist women and HCPs to identify specific problems. For example, the 19-item Female Sexual Function Index (FSFI; Rosen et al, 2000) or the Decreased Sexual Desire Screener (DSDS; Clayton et al, 2018) could be incorporated into diabetes consultations (see Appendix).
Supporting routine clinical enquiry
Implementing a clinical template within GP electronic records could support routine discussions around sexual well-being. For example, adding an automated prompt or a coded section under “Lifestyle” or “Quality of Life,” such as a tick-box for “sexual dysfunction discussion,” may encourage HCPs to address and document this more consistently. Embedding this within the clinical template is likely to increase the frequency of both enquiry and documentation by HCPs.
Management considerations
- Optimisation of lifestyle factors where appropriate (e.g. smoking cessation, weight loss).
- Optimisation of glycaemic levels.
- Use of gels and lubrication for any vaginal dryness.
- Provision of education on the difference between vaginal lubricants and moisturisers, alongside information on products available through the NHS, is essential. This includes raising awareness of over-the-counter options and identifying products marketed towards women that may be unsuitable. This supports safer and more informed choices.
- Psychological interventions.
- Pharmacological treatments for sexual dysfunction in women with diabetes, such as PDE5 (phosphodiesterase type 5) inhibitors, have shown some improvement in sexual arousal. However, the evidence remains limited, as many studies have methodological weaknesses, including the use of non-validated outcome measures, small sample sizes and the absence of appropriate control groups (Winkley et al, 2021).
- The use of hormone replacement therapy (HRT), including vaginal HRT where clinically appropriate, may support the management of symptoms such as vaginal dryness and recurrent urinary tract infections (UTIs). Recurrent UTIs or pain associated with sexual activity may have a significant psychological impact, potentially reducing a woman’s desire for intimacy or willingness to engage in sexual activity.
- Reviewing a woman’s contraceptive method and current medications is important when assessing sexual dysfunction. Medications used to manage diabetes and other chronic conditions, such as hypertension or depression, as well as over-the-counter therapies, may contribute to adverse effects including reduced libido, recurrent UTIs, vaginal thrush or genital dermatological symptoms.
- Beyond standard management approaches, there are FDA-approved pelvic health devices designed to support conditions such as vaginal tightness, pelvic pain and dyspareunia. These include vaginal dilators, vaginal weights, pelvic wands and rectal dilators. However, unlike devices and treatments available for men in the management of erectile dysfunction, these interventions are not routinely prescribed or funded through the NHS. If future women’s health initiatives and policy agendas in the UK provide greater recognition and support for female sexual health, specialist HCPs may be better positioned to advocate for, recommend or prescribe these interventions, where clinically appropriate.
Appendix



How the needs of people with a mental health problem and diabetes can be met.
29 May 2026