

Diabetes technology is transforming the management of type 1 diabetes in children and young people (CYP). National guidance now supports wider use of continuous glucose monitoring (CGM) and hybrid closed-loop (HCL) systems to improve glycaemic outcomes and quality of life (NICE, 2023a; 2023b). Despite this progress, inequalities in access persist, particularly among families affected by deprivation, language barriers and digital exclusion. This article describes a practical service redesign within a large paediatric diabetes team aimed at improving equitable access to diabetes technology through workforce innovation, structured education and targeted outreach.
Identifying inequalities in technology uptake
North West Anglia NHS Foundation Trust supports a large and geographically diverse CYP diabetes population across multiple counties. As the paediatric service expanded rapidly following increasing adoption of diabetes technology, variation in technology uptake became increasingly apparent across the caseload.
A review of local service data identified lower uptake and engagement with CGM and HCL systems among:
- Families living in areas of higher deprivation.
- Families in which English was not the first language.
- Families with lower digital confidence.
- CYP requiring additional educational support.
Families also described challenges attending appointments, understanding technology information and accessing ongoing support. Traditional clinic-based education models were becoming increasingly difficult to sustain owing to workforce pressures and growing service demand.
These findings highlighted the need for a more flexible and inclusive model of care that could better support underserved populations and reduce barriers to accessing diabetes technology.
Service redesign and interventions
Workforce innovation
Two dedicated support roles were introduced within the multidisciplinary team:
- Paediatric Diabetes Care Technician (PDCT).
- Paediatric Diabetes Clinical Educator (PDCE).
These roles focused on:
- Technology onboarding.
- Device troubleshooting.
- Structured patient education.
The introduction of these posts improved service capacity and enabled more consistent delivery of education while releasing specialist nurse time for complex clinical care.
Structured education pathways
Standardised education pathways were developed to improve consistency and accessibility across the service. Resources included:
- Pump workbooks.
- Step-by-step onboarding guides.
- Visual educational materials.
- Resources translated into various languages.
Education delivery was adapted according to family need using a combination of group sessions, individual appointments and virtual support.
Community engagement and outreach
To improve engagement with underserved groups, the service introduced:
- Community technology roadshows.
- Flexible education appointments.
- Opportunistic support outside traditional clinic settings.
This enabled families to access support in more accessible and less formal environments, helping to build confidence and trust in diabetes technology.
Addressing digital exclusion
A “poverty proofing” approach was incorporated into service delivery. Consideration was given to:
- Access to compatible devices.
- Internet and data limitations.
- Digital literacy.
- Practical barriers affecting attendance and engagement.
The focus shifted from expecting families to adapt to the service towards adapting the service around family needs.
Outcomes
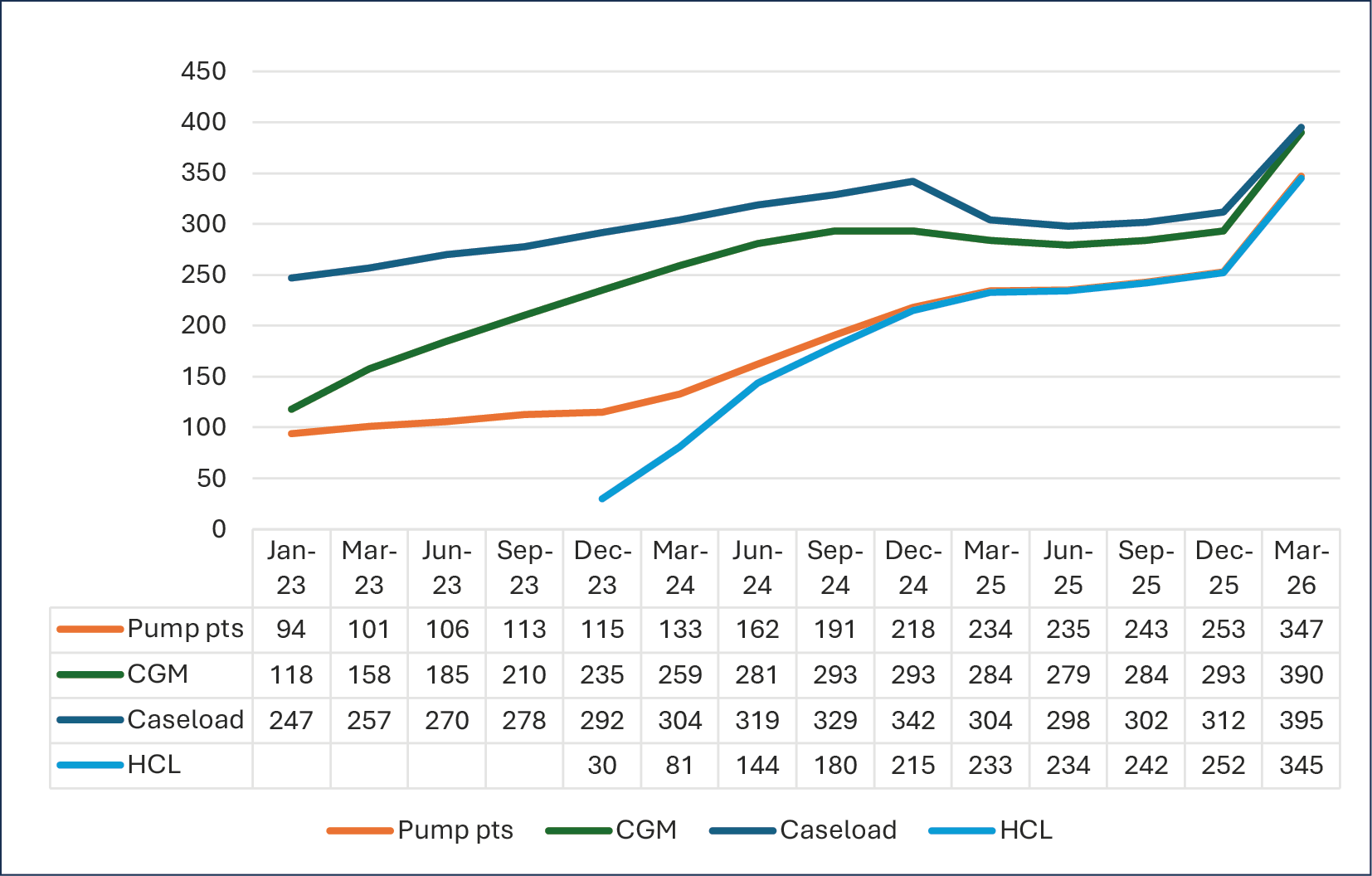
Following implementation of the programme, uptake of diabetes technology increased significantly across the service.
CGM uptake increased from approximately 48% of the caseload in January 2023 to almost 99% by March 2026. HCL uptake also increased substantially, from approximately 12% to 87% during the same period (Figure 1).
Engagement improved among previously underrepresented groups, and families reported increased confidence using diabetes technology as part of routine diabetes management.
The service also observed:
- Improved efficiency within clinic appointments.
- Greater consistency in education delivery.
- Increased staff capacity for complex clinical support.
At the time of review, the majority of CYP within the service were using diabetes technology as part of routine care, reflecting national ambitions to improve equitable access to diabetes technologies for all eligible children and young people (NICE, 2023a).
Implications for practice
Many of the challenges identified within paediatric diabetes services are also increasingly recognised within adult diabetes care. Workforce pressures, digital exclusion and inequalities in technology uptake affect services across all areas of diabetes management.
Although local populations and resources vary, several principles underpinning this project are transferable:
- Flexible education models.
- Dedicated support roles.
- Proactive outreach.
- Tailored communication strategies.
- Data-driven service improvement.
Embedding these approaches into routine practice may help reduce inequalities and improve equitable access to diabetes technology across wider diabetes services.
| Key points. |
| • Dedicated education and support roles can improve service capacity and patient engagement. • Structured technology pathways reduce variation in care delivery. • Community outreach improves access for underserved populations. • Digital exclusion should be considered routinely within diabetes service planning. • Local data can help identify inequalities and target interventions effectively. |
Conclusion
Improving equitable access to diabetes technology requires more than increasing the availability of devices alone. Services must also address the practical, educational and social barriers that influence engagement and uptake.
This quality improvement initiative demonstrated that workforce innovation, accessible education and proactive outreach can significantly improve equitable access to diabetes technology for CYP with type 1 diabetes. The learning from this work may support other diabetes teams seeking to reduce inequalities and improve technology uptake within their own services.



Developments that will impact your practice.
25 Jun 2026