

Type 2 diabetes currently affects 7% of the total population in the UK, with a new diagnosis made every two minutes (Whicher et al, 2020). The prevalence has doubled over the past 20 years, with 4.7 million people now affected. This figure is projected to rise to 5.5 million by 2030, equating to around one in ten adults (Diabetes UK, 2024). The economic burden of diabetes is substantial, accounting for approximately 10% of total NHS expenditure, highlighting the need for cost-effective interventions to improve glycaemic control and reduce complications (Hex et al, 2012).
The long-term effects of type 2 diabetes are well documented and include microvascular complications, such as retinopathy, neuropathy and nephropathy, as well as macrovascular disease (Fowler, 2008). The condition is thought to contribute to 530 myocardial infarctions each week in the UK (NHS Digital, 2016), and approximately 18% of hospital beds are occupied by patients with diabetes (NHS Digital, 2020). Hospital stays tend to be longer for people with diabetes, increasing the risk of medication errors and healthcare costs, and negatively impacting on individuals’ ability to self-manage their condition (Flanagan et al, 2018).
Evidence demonstrates that optimising diabetes control helps to prevent long-term complications (UK Prospective Diabetes Study Group, 1998). These findings underscore the importance of embedding diabetes self-management education (DSME) within routine care to optimise long-term outcomes and reduce the burden on the NHS. Structured education programmes for people with type 2 diabetes are considered an integral part of diabetes care and should be delivered following diagnosis, meeting the individual’s cultural, linguistic, cognitive and literacy needs (NICE, 2023).
There is a wealth of evidence validating the benefits of group-based DSME compared with routine care for people with type 2 diabetes (Steinsbekk et al, 2012). UK studies demonstrate that structured self-management programmes, including education and digital interventions, empower individuals to take an active role in managing their condition and result in modest but clinically meaningful improvements in HbA1c (2.2–6.6 mmol/mol) at 6 months post-intervention. The most effective programmes are multi-component and involve enhanced contact time (>10 hours; Captieux et al, 2018).
There are several diabetes self-management programmes available in the UK, including DESMOND (Diabetes Education and Self-Management for Ongoing and Newly Diagnosed), the X-PERT Diabetes Programme and, locally in Dorset, the N2T2 (New to Type 2) education programme and REFOCUS (On Your Diabetes). Over time, the delivery of these programmes has diversified, with provision offered in both group and digital formats to accommodate varying patient needs and preferences.
Research indicates that these multi-component educational interventions can improve patient knowledge, psychosocial outcomes and health behaviours, although statistically significant improvements in HbA1c are not universally reported (Deakin et al, 2006; Khunti et al, 2012; Chatterjee et al, 2018). Evidence from the DESMOND and X-PERT trials demonstrates improvements in illness beliefs, empowerment and lifestyle behaviours, with modest but clinically relevant reductions in HbA1c in some cohorts (Deakin et al, 2006; Khunti et al, 2012; Wheatley et al, 2021). Locally developed programmes, such as N2T2, align with these principles, aiming to provide accessible education soon after diagnosis (Wheatley et al, 2021). However, while these programmes often discuss and promote increased physical activity, there is limited evidence of the effectiveness of those that include structured exercise as part of the programme.
The management of chronic diseases such as cardiovascular disease and chronic obstructive pulmonary disease has shown improved outcomes following the implementation of rehabilitation programmes (Richardson et al, 2019). Exercise and increasing physical activity, alongside improvements in lifestyle and diet, are key components of both cardiac and pulmonary rehabilitation programmes. Physical activity, including planned and unplanned exercise, has been shown to greatly improve health outcomes and glycaemic management of individuals of all ages with type 2 diabetes (Kanaley et al, 2022).
However, people with type 2 diabetes are less likely to engage in physical activity than the general population (Morrato et al, 2007). A recent trial evaluating a structured exercise programme for people with type 2 diabetes demonstrated improvements in HbA1c, although these did not reach statistical significance (Mukherji et al, 2022). Notably, this trial did not include dietary or other interventions that would typically form part of a rehabilitation programme.
Refocusise: a new service intervention
The Refocusise programme was developed to support people living with type 2 diabetes to improve the management of their condition while engaging in regular exercise. The programme is run weekly from the Bournemouth Heart Club (BHC) and is supported by one diabetes specialist nurse from University Hospitals Dorset and two exercise therapists from the BHC. To date, twelve courses have been completed, with group sizes ranging from 11–15 participants.
Anyone with type 2 diabetes who wants to participate can be referred by their GP or practice nurse. They are subsequently invited to enrol in the 8-week course that combines structured exercise sessions with an established DSME programme at the BHC. Baseline and post-intervention assessments are undertaken and include HbA1c, blood pressure, body mass index, waist circumference, lipid profile and psychological well-being (using the Hospital Anxiety and Depression Scale [HADS]).
On completion of the course, participants are invited to join the BHC or are encouraged to continue with other forms of structured exercise. HbA1c is reassessed at 1-year and 2-year follow-up to evaluate long-term glycaemic outcomes. As this is a service evaluation, NHS ethical approval was not required. Participants consented for their data to be collected to enable evaluation of the service.
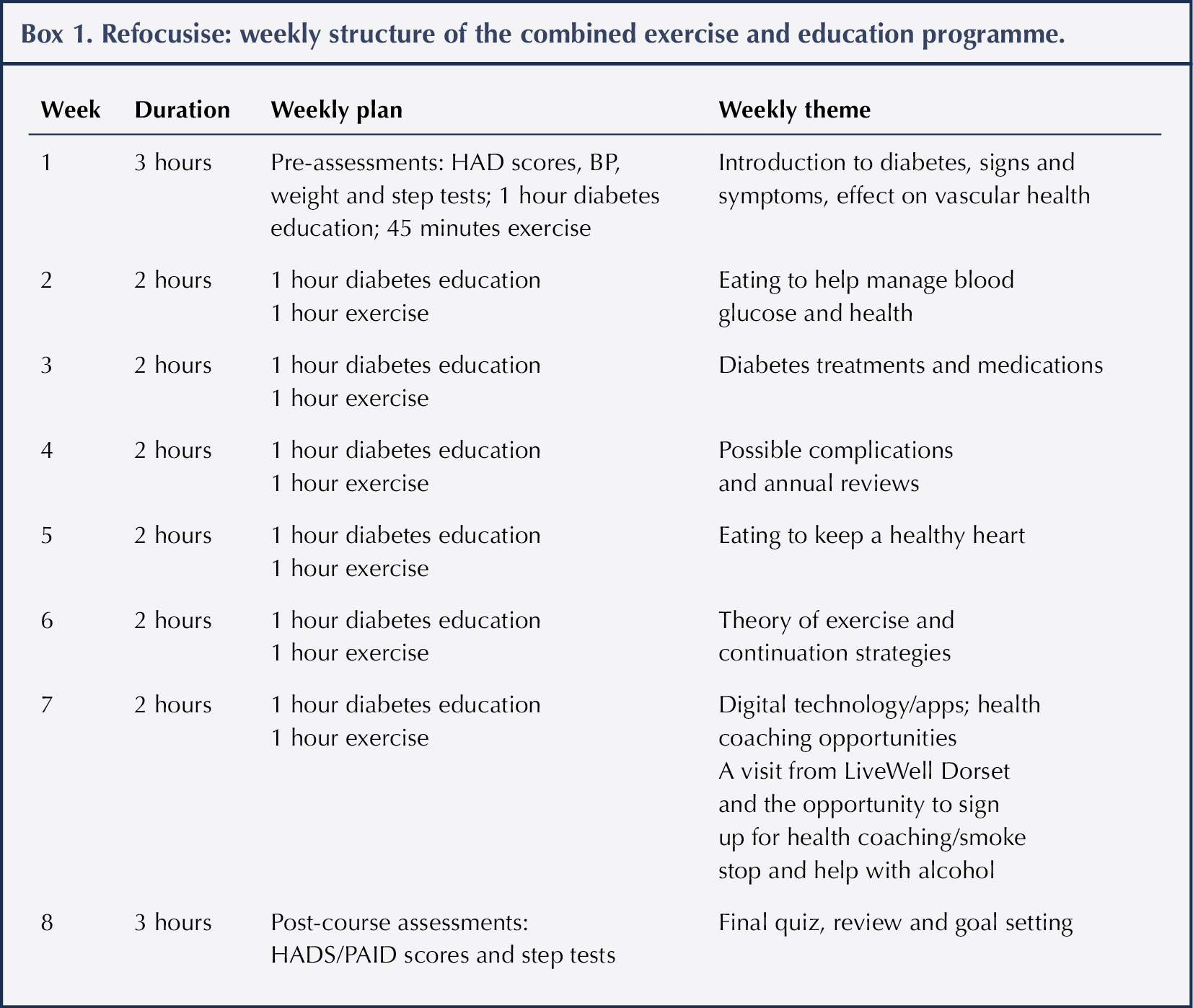
The exercise component of the Refocusise course incorporates a carefully structured, progressive circuit designed to enhance cardiovascular health while promoting overall functional strength in both the upper and lower body (Box 1). To ensure inclusivity, the circuit accommodates participants of varying abilities by offering both seated and standing exercise options, enabling individuals to engage at a level aligned with their comfort and capacity each week.
Specialist instructors deliver multiple intensity variations for each exercise, supporting gradual progression while preventing overexertion. Each movement includes weighted and body-weight alternatives, with clear demonstrations of how exercises can be modified to increase or decrease intensity as required.
Over the 8-week duration of the programme, the number of exercises performed is expanded to match participants’ improving fitness levels. Higher-intensity options are introduced for those ready to progress, while individuals who begin with seated exercises are encouraged to transition toward standing positions where appropriate, fostering safe and sustainable advancement.
Results
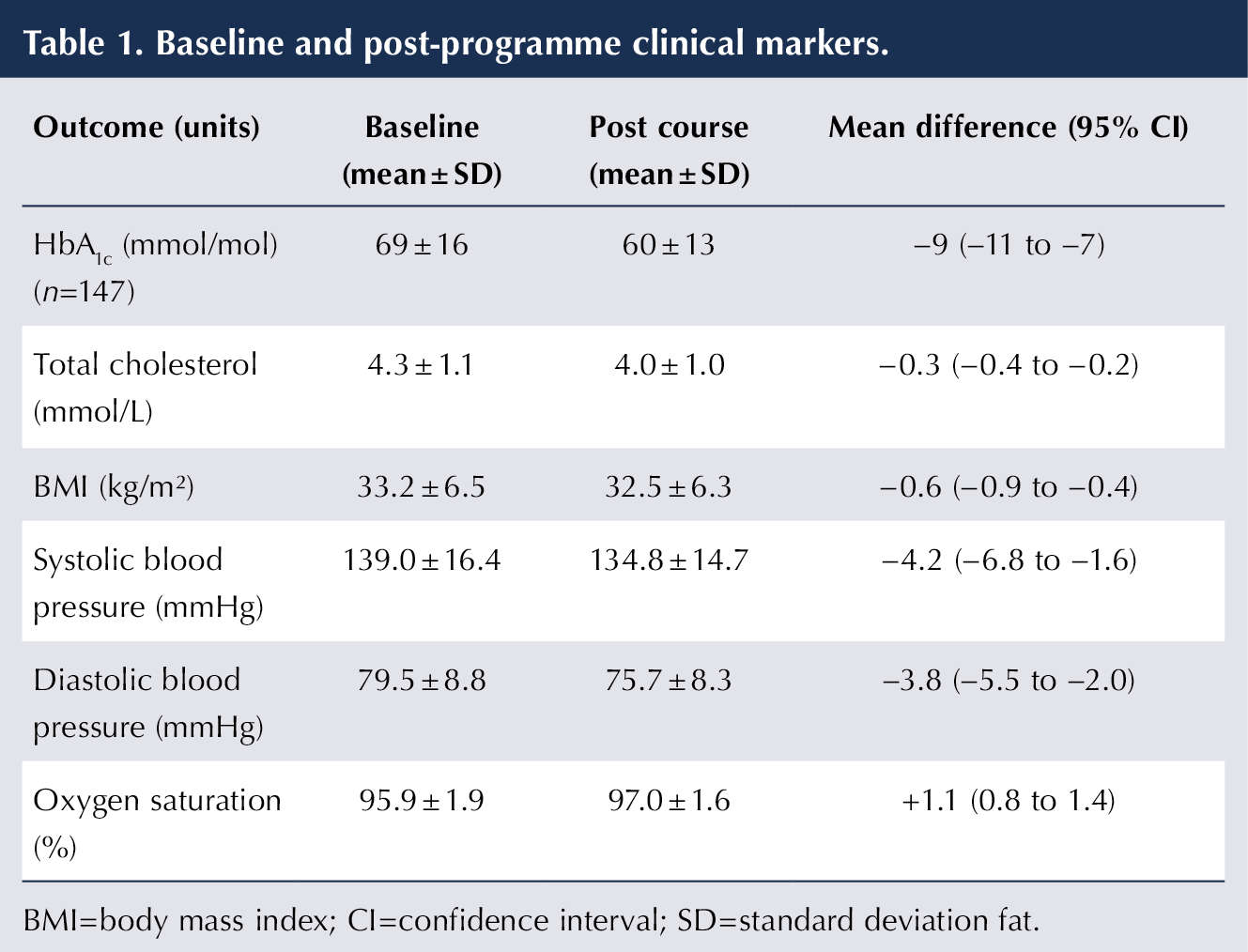
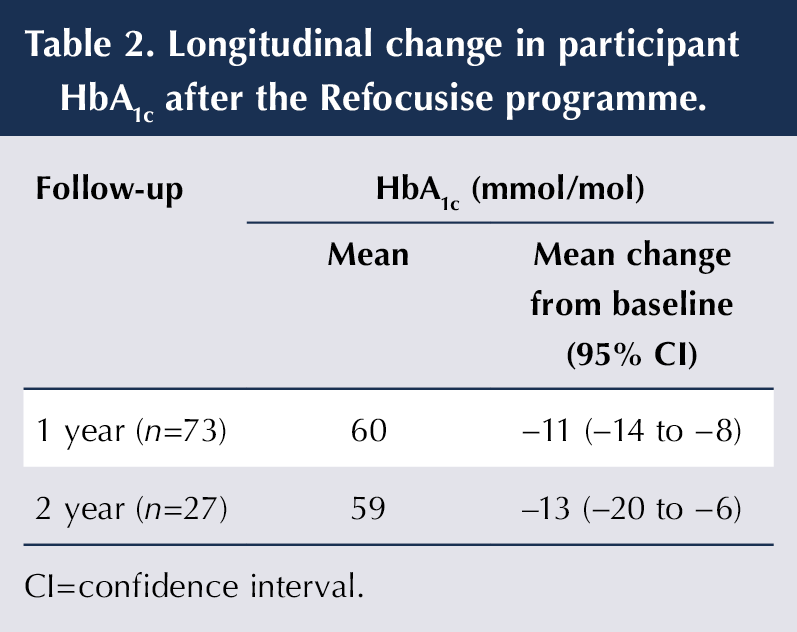
The programme has been completed by 147 people (74 males), with a mean age of 64 years (range, 23–84 years). Initial results following the intervention have been positive, with improvements observed across all clinical markers (Table 1). These benefits were sustained over the longer term, with a mean reduction in HbA1c of 11 mmol/mol at 1-year follow-up (n=73), which was maintained at 2 years following the intervention (Table 2).
Furthermore, the participants demonstrated improvements in mental wellbeing, as reflected in their HADS scores. Eighty-three participants completed the HADS at baseline and after programme completion. At baseline, the mean anxiety (HADS-A) score was 7.3 (SD, 4.2; range, 0–16), and the mean depression (HADS-D) score was 5.23 (SD, 3.1; range, 0–14). Post-programme, the mean anxiety score decreased to 5.8 (SD, 3.8; range, 0–16) and mean depression score to 3.6 (SD, 2.9; range, 0–10). HADS scores of 8–10 indicate mild anxiety or depression, 11–14 moderate and 15–21 severe symptoms (NICE, 2025).
Participants also provided written feedback describing the impact of the programme on their health and lives. One participant described Refocusise as “the start of the rest of your life”, while another reported that “This course has changed the way I think about diabetes.” Improvements in physical health associated with the exercise component were recognised through comments such as “My knees have improved” and “I can move my shoulder again”. Improvements in mental wellbeing were also noted, with comments such as “Everyone says I’m happier” and “I can play with the grandchildren more easily.”
Discussion
Evidence demonstrates that chronic disease management programmes (CDMPs) can positively impact the lives of people living with long-term conditions (Gbigbi-Jackson et al, 2024). Exercise-based cardiac rehabilitation is associated with reductions in cardiovascular mortality and hospitalisations, alongside improvements in quality of life (Dibben et al, 2023). Comparable benefits have been observed in exercise-based pulmonary rehabilitation, including improvements in respiratory symptoms and overall wellbeing (McCarthy et al, 2015).
Exercise is also a fundamental component of diabetes self-management. Both the American Diabetes Association (Colberg et al, 2016) and NICE (2026) recommend daily physical activity as a key lifestyle modification to support optimal diabetes control. Despite this, adults with type 2 diabetes often report higher levels of sedentary behaviour and lower engagement in physical activity compared to those without the condition (Kennerly and Kirk, 2018). Following completion of the Refocusise programme, a number of participants have joined the Bournemouth Heart Club and have continued to exercise on a regular basis, suggesting that participation may support longer-term engagement in physical activity.
The initial outcomes from the Refocusise programme indicate improvements across all measured clinical markers. Notably, the sustained reduction in HbA1c suggests that this intervention may confer health benefits and, potentially, economic advantages. Evidence consistently shows that improved glycaemic control in people with diabetes is associated with significant cost savings, as even modest reductions in HbA1c can reduce complications and subsequent healthcare expenditure (Baxter et al, 2016). Collectively, these findings reinforce the premise that early intervention and preventative strategies can be both clinically effective and economically beneficial.
The primary aim of Refocusise is to improve glycaemic control and promote holistic health and wellbeing in people with diabetes. Findings from this service evaluation suggest that these objectives were achieved within this small cohort. The next step is to extend the programme to a larger and more diverse population to determine whether these outcomes can be replicated. This approach aligns with a Diabetes UK position statement emphasising the need for research into integrating structured exercise into diabetes care, drawing on established cardiac and pulmonary rehabilitation models (Morris et al, 2023).
Limitations
This service evaluation involved a small sample of participants who were referred by their GP and were aware that the programme included exercise, introducing a potential element of selection bias. Furthermore, the exercise programme was delivered by highly experienced staff at the Bournemouth Heart Club, a specialist facility that may not be accessible to the wider population should the intervention be scaled up. While the results are promising, they are derived from a relatively small and specific cohort. Future research should evaluate the effectiveness of this model in larger, more diverse cohorts and across different healthcare settings.
Conclusion
This service evaluation indicates that incorporating structured exercise into an enhanced diabetes self-management education programme can result in clinically meaningful improvements in glycaemic control, cardiovascular risk factors and psychological well-being. These benefits were observed immediately following programme completion and were sustained at one and two years. The findings support the integration and wider implementation of combined exercise and education interventions within routine diabetes care.



Developments that will impact your practice.
30 Apr 2026