
ADA/EASD Consensus on type 1 diabetes management launched
Following the sharing of the draft guidance at the ADA Scientific Sessions earlier this year, the joint ADA/EASD Consensus Report on the management of type 1 diabetes in adults was published in Diabetes Care and Diabetologia to coincide with the EASD meeting. The report was influenced by the ADA/EASD consensus on type 2 diabetes management, and the authors acknowledged that there was a need to develop a comparable guideline that specifically addresses the needs of people with type 1 diabetes.
The unifying concept of the report is personalised care, meeting the needs of the person with type 1 diabetes, including optimising insulin therapy as safely as possible, and taking into account the individual’s preferences, comorbidities, capabilities, health status, and social and other circumstances (see Figure 1).
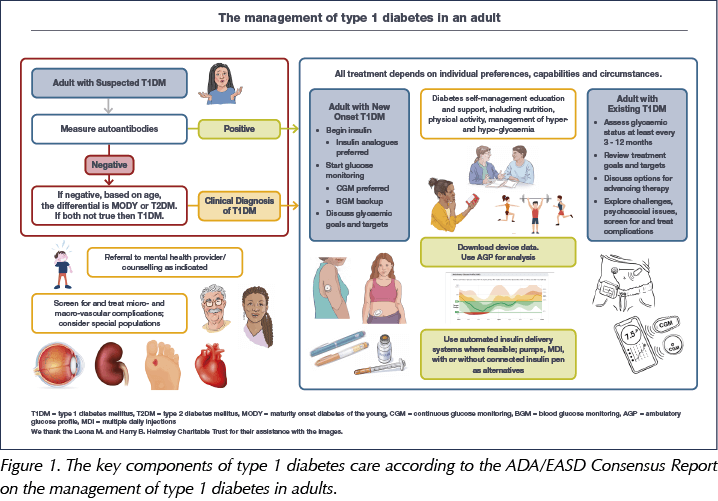
Important highlights include an algorithm to accurately diagnose type 1 diabetes, since no single factor in isolation can reliably confirm the condition. Some 40% of individuals diagnosed with type 1 diabetes as adults are initially misdiagnosed as having type 2 diabetes, partly because the latter is becoming more common in younger adults.
To achieve individualised care, a needs assessment should precede diabetes self-management education and support from the healthcare team, and four critical times for ongoing education are identified: at diagnosis; annually and/or when the person is not meeting treatment targets; when complicating factors develop; and when transitions in life and healthcare occur.
The report also addresses behaviour considerations such as alcohol and tobacco use, sleep, sick day management, driving, employment, physical activity and nutrition. As with treatment, nutrition advice needs to be individualised; no single eating pattern is recommended.
Continuous glucose monitoring (CGM) is advised as the standard of care for glucose monitoring in adults with type 1 diabetes, although the choice of device should be determined by the individual’s preferences and needs. Multiple daily injections or continuous subcutaneous infusion are recommended as the insulin regimens of choice. Structured education, CGM and automated insulin delivery are all crucial to lowering HbA1c without increasing the occurrence of hypoglycaemia.
With 20–40% of people with type 1 diabetes experiencing high levels of emotional distress related to the condition (including 15% with depression), the guidance supports periodic patient screening for self-management difficulties and psychological and social problems.
The report also covers diabetic ketoacidosis, inpatient care, adjunct therapies, pregnancy, pancreas and islet cell transplantation, and treatment individualisation in older age. It is full of support materials, including tables on the following:
- Glycaemic targets
- Schedules of care
- Key content of diabetes education
- Non-glycaemic factors that can alter HbA1c
- Examples of subcutaneous insulin regimens
- Properties of approved and non-approved adjunct therapies, including metformin, pramlintide, GLP-1 RAs and SGLT2 inhibitors.
Click here to read the guidance in full.
DAPA-CKD: Subanalyses show further benefits
Data from prespecified subanalyses of the DAPA-CKD trial of dapagliflozin for the treatment of chronic kidney disease (CKD) were presented, showing that the SGLT2 inhibitor reduced the incidence of type 2 diabetes in those without the condition at baseline by 33% compared with placebo. This was a similar risk reduction to the 32% reduction observed in the DAPA-HF trial in those with heart failure.
Further analysis of renal outcomes also suggested that the agent was effective in reducing the primary renal endpoint (sustained ≥50% reduction in eGFR, end-stage renal disease, or death from cardiovascular or kidney disease) across the CKD stages, with similar benefits in those with stage 4 CKD at baseline as in those with stage 2–3 disease.
Safety analyses suggested that the risk of acute kidney injury (AKI) was significantly lower in dapagliflozin recipients, despite the initial eGFR reduction that is typically seen when initiating all SGLT2 inhibitors. This is reassuring and strengthens the case for not checking the eGFR 2 weeks after initiating dapagliflozin, and instead checking it with other blood tests such as HbA1c at 3–4 months. However, if the patient is deemed prone to dehydration then it remains appropriate to check earlier after initiation, and to stop the drug and reconsider if the eGFR has dropped by more than 30%.
Subanalysis of cardiovascular outcomes showed that the presence of heart failure, peripheral arterial disease and/or atrial fibrillation as comorbidities in those with CKD did not alter the effectiveness of dapagliflozin, although unsurprisingly they did increase the risk of cardiovascular mortality and hospitalisation for heart failure significantly.
ReTUNE trial: Intensive weight loss can achieve type 2 diabetes remission even in those with a normal BMI
Previously, the landmark DiRECT (Diabetes Remission Clinical Trial) study showed that an intensive weight loss programme delivered by GPs can put type 2 diabetes into remission in people who are overweight. Now, preliminary results from the ReTUNE (Reversal of Type 2 Diabetes upon Normalisation of Energy Intake in the Non-obese) trial indicate that the programme can also reverse the condition in people of normal weight.
Twelve people with type 2 diabetes despite having a normal BMI (<27 kg/m2; mean, 24.5 kg/m2) followed an 800 kcal/day soups-and-shakes diet for two weeks, followed by 4–6 weeks in which they received support to maintain their new weight. They completed up to three rounds of this diet/maintenance cycle until they had lost 10–15% of their body weight. Eight of the 12 participants (67%) achieved type 2 diabetes remission (HbA1c <48 mmol/mol whilst off any diabetes medication). Average weight fell by 8.2 kg (11.9%), while total body fat fell from 33.1% to 27.4%.
The participants were also compared with 11 control subjects without diabetes, matched for age, sex and (post-weight-loss) BMI. Following weight loss, their levels of body fat, liver and pancreatic fat, and plasma triglycerides had all fallen significantly and were similar or approaching levels seen in the controls.
In the population at large, approximately 10% of people with type 2 diabetes have what is viewed as a healthy BMI. Professor Roy Taylor (Newcastle University), lead author of the ReTUNE and DiRECT studies, commented: “These results, while preliminary, demonstrate very clearly that diabetes is not caused by obesity but by being too heavy for your own body. It’s due to having too much fat in your liver and pancreas, whatever your BMI.”
A new focus on obesity management in type 2 and type 1 diabetes
Speaking at the shared EASD/Lancet symposium on obesity, Ildiko Lingvay (UT Southwestern Medical Center, Dallas, TX, USA) and colleagues spoke of a need to focus on weight loss of at least 15% as the cornerstone of management for the majority of people with type 2 diabetes. Although managing glycaemia and cardiovascular/renal risk will inevitably be a key part of management also, it was argued that focusing on significant weight loss early would have a cascade of benefits on insulin resistance and subsequent diabetes complications.
The authors argued that data from DiRECT and ReTUNE show that intensive dietary interventions can result in “double-digit” weight loss and even type 2 diabetes remission, and recent advances in drugs with weight-lowering effects mean that this weight loss is now more achievable than previously. Thus, they concluded:
“The time is right to consider the addition of substantial (i.e. double-digit %) weight loss as a principal target for the treatment of many patients with type 2 diabetes. This approach would address the pathophysiology of the disease process for type 2 diabetes; recognise adipose tissue pathology as a key underlying driver of the continuum of obesity, type 2 diabetes, and cardiovascular disease; and reap metabolic benefits far beyond blood sugar control. Such a change in treatment goals would recognise obesity as a disease with reversible complications and require a shift in clinical care.”
Dr Lingvay added, “Healthcare providers, especially those managing people with diabetes routinely, should be trained and become experienced in all aspects of obesity management. Support staff should be trained to support patients through their weight-loss journeys, and practices should consider the need for specialised staff to deliver the educational component of the new treatment strategies that are proposed.”
Type 1 diabetes and obesity management
Later in the same symposium, Bart Van der Schueren (University Hospitals Leuven, Belgium) and colleagues argued that we should not forget to address the issue of obesity in people with type 1 diabetes, who are also being hit by the global obesity pandemic; indeed, there is some evidence that obesity rates are growing more quickly in this group than in the general population. Not only are exogenous insulin injections likely to result in more weight gain than normal physiological insulin secretion, but people with type 1 diabetes may often feel the need to consume superfluous calories in order to avoid hypoglycaemia when undertaking certain activities and exercise. Following calorie-restricted diet plans for weight loss may also be more difficult if hypoglycaemia is a concern.
Unfortunately, specific goals and strategies do not yet exist regarding weight management in people with type 1 diabetes. One of the most effective strategies for preventing weight gain has proven to be the provision of additional nutrition education, which allows for more accurate tailoring of insulin doses to levels that mimic physiological levels. However, resources to provide such education are lacking in many settings. Adjunct therapies, such as metformin, GLP-1 receptor agonists, SGLT2 inhibitors and the amylin analogue pramlintide, may also play a helpful part. However, they can have side effects which must be taken into consideration. Obesity surgery was also discussed; however, while this can massively reduce the complications of obesity in people with type 1 diabetes, it can also increase the risk of hypoglycaemia and substance abuse.
The authors call for more research to get a better grasp of the exact prevalence of the abnormal and/or excessive accumulation of body fat in people living with type 1 diabetes, which eventually leads to overweight and obesity, to understand if and how these processes differ from people in the general population.
Common osteoporosis drug may reduce risk of type 2 diabetes
Data from Denmark suggest that the widely used osteoporosis drug alendronate reduces the risk of developing type 2 diabetes. Alendronate is a bisphosphonate and is used first-line to help strengthen bones and reduce the risk of a fracture in people with osteoporosis.
Dr Rikke Viggers (Aalborg University Hospital, Denmark) conducted a retrospective, case–control study using Danish national registry records and compared 163 588 people with type 2 diabetes and 490 764 matched controls without the condition. Over a 10-year follow-up period, the crude odds ratio (OR) of developing type 2 diabetes after alendronate use was 0.93 (95% confidence interval [CI], 0.90–0.96). After adjustment for other factors associated with type 2 diabetes, including smoking, obesity and steroid therapy, the OR reduced further to 0.64 (95% CI, 0.62–0.66).
The adjusted risk was reduced by 53% in those with more than 8 years of alendronate use, and there was evidence of a dose–response relationship between longer effective use of alendronate and lower risk of type 2 diabetes.
While it is not yet clear how alendronate reduces the risk of developing type 2 diabetes, one hypothesis is that the drug reduces low-grade inflammation and oxidative stress, two processes thought to be central to the development of insulin resistance.
The material has been peer reviewed by the congress selection committee. It has been submitted to a medical journal but the full paper is not yet available.
Almost 4 million HbA1c tests likely to have been missed or delayed during the pandemic
Estimates extrapolated from test sites across the UK suggest that there were 3.9 million fewer HbA1c tests conducted over the first 6 months of the pandemic compared with the average over the same time period in previous years. This includes 2.5 million diagnostic tests, which likely led to 213 000 cases of prediabetes and 68 500 cases of diabetes going undiagnosed.
Among people with pre-existing diabetes, an estimated 1.4 million monitoring tests were missed or delayed, including over 500 000 in people with high blood glucose levels. Results suggest that this delay in monitoring was linked to an average increase in HbA1c of 2–3 mmol/mol. Commenting on the findings, the lead study author, David Holland (Director, The Benchmarking Partnership), said: “Even now, in September 2021, HbA1c test volumes are only just starting to reach the levels we would typically expect to see. The impact may last well beyond the crisis, potentially creating long-term health repercussions and placing new demands on an already overburdened NHS. The healthcare system urgently needs to find a way to test and review the most at-risk [people with diabetes] before the increased risks they face to their long-term health become a reality.”


Genetic deficiency is more prevalent in Black and South Asian individuals, raising concerns about diabetes outcomes.
1 Oct 2025