

Diabetes is a lifelong condition that carries a risk of acute and chronic complications if poorly controlled for a long period. To manage type 1 diabetes effectively, individuals using multiple daily injection (MDI) or standard pump therapy must make numerous decisions across every 24-hour period (Griffin et al, 2023). Hybrid closed-loop (HCL) systems, directed by an algorithm and using values from a continuous glucose monitor, adjust insulin delivery every 5–12 minutes. This technology can improve glycaemic outcomes and significantly reduce the management burden for those living with type 1 diabetes (Zeng et al, 2023; Ng et al, 2024).
Paediatric diabetes services are in the process of offering HCL systems to all children and young people (CYP) with type 1 diabetes in the UK as an option for the management of blood glucose levels (NICE, 2023; NHS England, 2024). In 2023–2024, 32,809 CYP with type 1 diabetes were cared for by paediatric diabetes services in England and Wales, with 54.8% using HCL systems (Royal College of Paediatrics and Child Health, 2024). To achieve maximal benefit from HCL systems, users need a good understanding of how to operate them, supported by the provision of comprehensive structured education (SE). The Association of British Clinical Diabetologists’ Diabetes Technology Network recommends that this should take 8 hours for those new to pump therapy and 4 hours for those upgrading from an existing pump (Griffin et al, 2023). Diabetes teams therefore face the challenge of effectively educating large numbers of CYP within a short period, enabling equitable and timely access to this transformational technology.
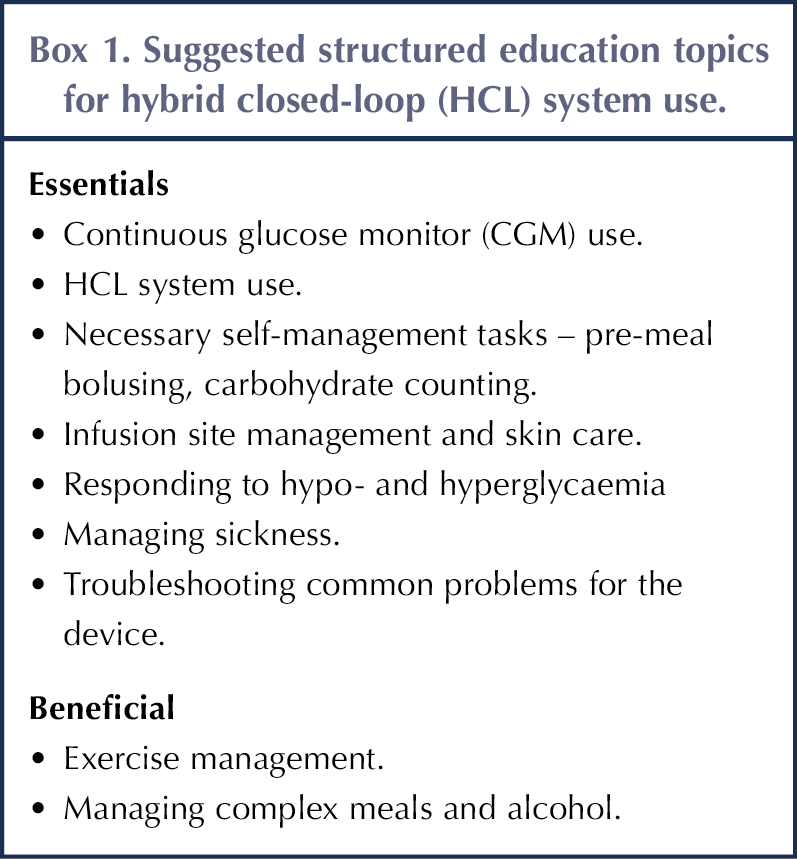
There are multiple HCL options available, with the main four being: CamAPS FX, MiniMed 780G, Omnipod 5 and t:slim X2 with Control IQ. Each uses different algorithms and advanced pump features. Structured education should cover general management principles (Box 1) and teach individual pump functionality. It should set realistic expectations regarding glycaemic outcomes and the level of user effort required for these systems to function optimally (Griffin et al, 2023).
Learning styles
People learn in different ways. Some find listening most helpful, others engage better through writing or through pictures and diagrams, whilst some prefer learning through doing (Fleming, 1995). Teaching is most effective when it incorporates all these learning styles (Othman and Amiruddin, 2010). Narrative communication, which conveys meaning through stories, can complement instructive teaching (Bell et al, 2021).
Effective education
There can be a difference between the message an educator thinks they have conveyed and the one that is actually interpreted. The use of medical and scientific terminology, without careful explanation, can result in feelings of bewilderment and despair, rather than knowledge and empowerment (Lawton et al, 2015). Understanding should not be assumed; instead, it should be assessed through conversation, working through scenarios or quizzes (Rosenshine, 2012).
Appropriate education
A CYP will require support from a carer who has a good understanding of how to operate their HCL system. Young children have limited understanding or ability to engage with the complex aspects of pump management, so teaching initially will need to be directed largely towards their carers. For older CYP, diabetes management should be undertaken in partnership with their carer (Gregory et al, 2022). Adolescence can be a particularly challenging time for diabetes care (Khadilkar and Oza, 2022). Promisingly, a recent review of young people transitioning from MDI to HCL systems observed a positive impact on diabetes outcomes, linked to a period of re-engagement (Wong et al, 2024). SE delivered by educators skilled in engaging effectively with this age group may help to optimise this.
Accessible education
The Equality Act (2010) requires reasonable adjustments to be made for CYP and carers with additional needs, such as learning disabilities (LD) or autism. Resources should be adapted to suit personal communication skills and preferences, and Beresford (2022) references tools and methods that may support this. A CYP with LD may be supported by several carers, all of whom will require appropriate education.
Idkowiak et al (2023) observed that CYP requiring an interpreter had worse diabetes control up to 18 months after diagnosis compared with an equivalent group who did not require this support. To minimise health inequalities, SE needs to be provided in a way that overcomes cultural and language barriers. This includes offering diabetes-specific training for interpreters (Idkowiak et al, 2023), using the same interpreter across appointments and planning for the session to take twice as long (Office for Health Improvement and Disparities, 2021). Alongside professional translation services, online translation tools may be used informally by CYP and carers to overcome communication challenges, although effectiveness varies between languages and should be used very cautiously (Chen et al, 2016).
One-to-one education
In-person, one-to-one education has traditionally been how CYP are taught about diabetes (Lawal and Lawal, 2016). It allows for natural dialogue and the use of physical resources, and the pace can be set according to existing knowledge levels and ability, with understanding assessed through timely questions. This is, however, the most expensive type of education to deliver (Pemberton et al, 2024). To meet the demand from those wanting HCL systems, providing one-to-one education for everyone is likely to create a barrier to timely access. Nevertheless, some will require it, including CYP or carers with additional needs, mental health challenges or those requiring a translator.
Group education
Group education is widely used within adult diabetes services, where studies have shown it to be as effective as one-to-one teaching (Lawal and Lawal, 2016). Analysis of dietitians’ perspectives on group-based education for adults identified advantages, such as opportunities for patients to meet and share experiences, and to recognise that they are not alone. Challenges included managing group dynamics, such as people speaking over each other, dominating discussions or being unwilling to interact (Cairns and Sjöström, 2022).
iDEAL best practice guidance for group consultations in diabetes care recommends that similar individuals are grouped together to promote peer support (Holmes et al, 2022). In contrast, HCL system starts are often supported by a representative from one company, so are grouped by system choice.
Certain aspects of education are common to all HCL systems, so could be delivered to groups of similarly aged CYP using different systems, tailored to age-related needs. For example, SE for younger children could address unfinished meals and picky eating, whereas SE for older CYP could include management for competitive sport and alcohol use. This age-based approach could work well for SE that follows an initial system-led group start, once essential topics (see Box 1) have been covered.
Stephenson et al (2024) ran monthly play-centred clinics for children under 7 years of age, incorporating themed activities to support diabetes understanding. These provided peer support for the children, while carers learnt from one another. Ait-Taleb Lahsen et al (2024) delivered effective SE to groups of older CYP in three therapeutic educational sessions using PowerPoint presentations, brainstorming, role-play and discussion. Although such approaches require time and resources to create and run, in-person interactive group SE inspired by these methods might yield additional benefits, such as by providing a supportive space where children can play while parents learn, or where adolescents can interact.
Online education
Many trusts use virtual platforms, which can facilitate both individual and online group education (Akintomide et al, 2021). A key benefit of online appointments is that there is no travel, saving CYP and carers associated expenses, and reducing time out of school and work (Woodger et al, 2022). Older CYP may be able to attend from a room at school, while adults can join from different locations, which is an advantage for separated families or CYP with several carers.
Compared with in-person SE, online SE does not easily allow the use of physical resources, making it challenging to incorporate kinaesthetic learning. Asking attendees to interact safely with their pumps or pump simulators is one way to incorporate this. Online SE can utilise information from websites, HCL system data and PowerPoint slides, supporting learning through reading, images and listening.
Many paediatric diabetes services can access mobile phones for CYP who require them, which can also be used for online education. However, 16% of those aged over 15 years do not have basic digital literacy skills, and internet connections may be unreliable (Lloyds Bank, 2024). Should a CYP fail to attend, an educator should explore whether it may be because of such an issue.
Online appointments also risk attendees being disturbed by family life; if a quiet, confidential space cannot be found, face-to-face education may be necessary. Using a phone screen brings additional distractions, such as push notifications or calls. Giving instruction on expected engagement level, and assessing understanding after the session, can help educators determine whether learning outcomes have been met.
Presenting online group education sessions requires additional skills from the educator compared with in-person teaching. If there is only one educator, they must present the session, monitor interaction and attendance, and admit participants into the virtual room if they are late or need to re-enter. Challenging group dynamics can be managed with a “mute all” option, asking people to raise a virtual hand or inviting comments via a chatbox. Some attendees may feel unable or uncomfortable to be visible on camera (Castelli and Sarvary, 2021), making it hard for the presenter to gauge participation. Presenting sessions as a monologue risks disengagement; encouraging interaction, such as through the use of quizzes or polls, can help to address this (Maimaiti et al, 2023).
Flipped education
Technology using videos, apps and websites can provide SE without an educator present. A virtual flipped-learning SE programme for CYP starting HCL systems has been implemented (Pemberton et al, 2024). It provides step-by-step guides containing written information, pictures and videos, and finishes with a quiz. Pump onboarding was delivered in person, with two online group follow-up sessions. Compared with the previous method, which involved five face-to-face group sessions, the improvement in time in range was equivalent.
Benefits of this approach included reduced educator time and fewer clinic room requirements, whilst CYP could learn at a pace, time and place that suited them. Creating the programme cost around £4600, so it needed to onboard large numbers of children to be cost-effective.
Education for schools and colleges
Educational settings in the UK have a duty to provide appropriate care for CYP with diabetes, with designated members of staff being trained to do so by the diabetes team (Equality Act, 2010; Children and Families Act, 2014). Training is typically given in schools after a CYP has been diagnosed and at transition points when carers change (Goss et al, 2026).
The rapid shift of CYP onto HCL systems requires diabetes teams to update education for a significant number of staff in a relatively short timeframe. Whilst some in-person SE will be necessary, using online platforms, either individually or in groups, alongside pump simulators could enable the training of more people across multiple settings. Diabetes in Schools (DigiBete, 2026a), an online CPD-accredited platform, might complement this approach.
Supportive websites
All HCL systems have websites with supporting educational materials and training, which users are asked to complete before starting use. Some require assessments to be passed before access is granted. Content varies between companies and is directed at adults rather than children. Educators need to keep abreast of this, noting the risk that company education may not align with follow-up SE sessions that they deliver. Teams need to decide how much to rely on this content and how much independent SE to provide.
Examples of existing educational resources that support HCL use in CYP are outlined in Box 2. These include trusted digital tools, workbooks, guidelines and teaching aids, illustrating the range of materials available.
| Box 2. Resources available to support hybrid closed-loop (HCL) system education. |
DigiBete (2026b) is a free educational app and self-management platform for children and young people (CYP) with type 1 diabetes. It contains easy-to-understand short films about various aspects of diabetes care, alongside age-appropriate quizzes. Essential topics have been translated into 12 languages. The site offers extensive information about diabetes technology for those considering the use of a HCL system, with links to relevant websites. It provides videos and workbooks covering many aspects of diabetes management mentioned in Box 1, although these do not include pump-specific advice. Flipped-learning programme. To inspire other trusts, Pemberton et al (2024) provide the resources from their flipped-learning programme as supplementary material. Diabetes Technology Network-UK has a bank of resources and guidelines for HCL systems, although little for use with CYP. Panther Program provides healthcare professionals with practical resources on diabetes technology, including to help patient education. Information for adults includes guidance on skin care, managing hyperglycaemia and time in range (using mg/dL units). Physical activity and exercise. Moser et al (2025) present guidelines for HCL system use around physical activity, including pump-specific advice, using easy-to-read illustrations provided as slides in its supplementary information. Soft toys wearing diabetes tech, from Type One Style, can help demonstrate cannula or CGM site care. Pump companies share user stories from ambassadors on their social media accounts, providing a source of narrative input. There will be an element of promotion within these. Virtual quiz apps. Andriani et al (2023) review some applications commonly used to assess understanding. |
Conclusions
The challenge of providing SE to large numbers of CYP in a relatively short period is one that educators need to embrace creatively. Pump starts need to be done in person, providing an opportunity to deliver face-to-face education covering some key essentials. Online education has the potential to help meet increased demand, delivering SE especially on Beneficial Topics (Box 1).
Rapidly evolving technology, and the evidence base surrounding it, means that SE packages on the topic are few and not always up to date. Sharing of resources between trusts can reduce duplication, lower costs, encourage good practice and provide quality assurance.
There is a need for national quality assured SE programmes and a standardised approach. This may be something the National Children and Young People’s Diabetes Network could facilitate through a technology working group.
Acknowledgement
The author would like to acknowledge Birmingham City University’s Children and Young Person’s Diabetes Care Module.



Nicola Milne discusses how care is shifting to a more proactive, prevention-focused model.
22 Jul 2026