
Pressure ulcers are caused when an area of skin and the tissues beneath are damaged as a result of being placed under intense or prolonged pressure and/or shear forces sufficient to impair its blood supply (NICE, 2014; National Pressure Ulcer Advisory Panel, 2016). Even though the majority of hospital-acquired pressure ulcers are believed to be preventable, the incidence among patients in the UK and Europe remains high (Guy et al, 2013; Rajpaul and Acton, 2016; Guest et al, 2018), despite strategic drivers in place such as the NHS Safety Thermometer “harm-free” care initiative and CQUIN targets that promote a zero tolerance to healthcare-acquired pressure damage.
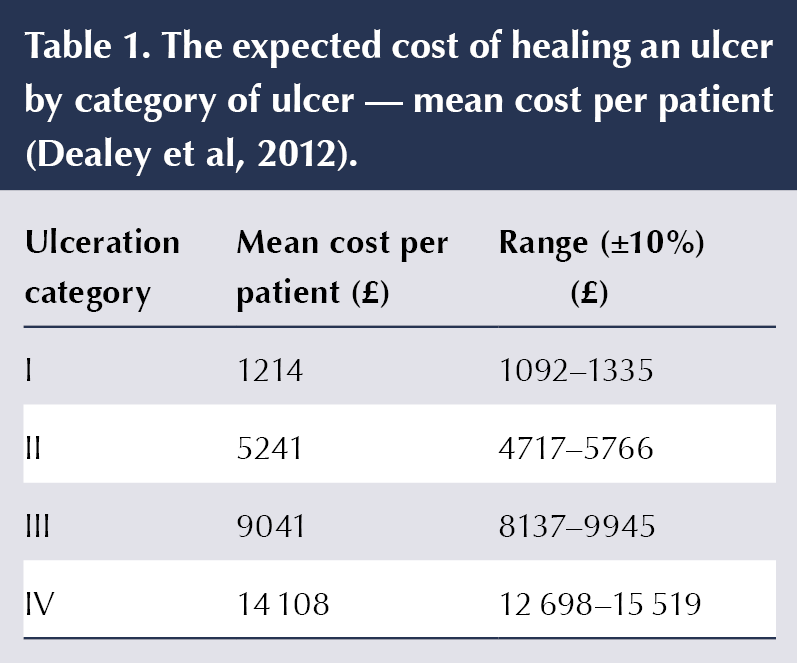
The cost of treating pressure ulcers in the UK ranges from £1214 for a category/stage 1 pressure ulcer to £14 108 for a category/stage 4 pressure ulcer, the costs increasing with pressure ulcer severity and the incidence of complications such as critical colonisation, cellulitis and osteomyelitis (Dealey et al, 2012). The cost to individuals is significant, with pain and distress (NICE, 2014), impacted quality of life (Franks et al, 2002; Spilsbury et al, 2007; Campbell, 2009; Gorecki et al, 2009; Repic and Ivanovic, 2014), loss of function (Lyder, 2011) and susceptibility to complications such as infection and osteomyelitis (Kerstein, 2002; Redelings et al, 2005; Lyder, 2011; Sullivan and Schoelles, 2013), which can sometimes result in lower-limb amputation and even death as possible outcomes (Kerstein, 2002; Brown, 2003; Redelings et al, 2005; Landi et al, 2007; Cook and Murphy, 2013; Rivolo, 2016). Other costs associated with the development of pressure ulcers include increased length of stay, increased hospital costs, the reputation of the hospital or care home and, even if the ulcers develop independent of good holistic care, potential litigation associated with hospital-acquired pressure ulceration (Lyder, 2011).
Heel pressure ulcers are the second most common site of pressure damage (Amlung et al, 2001; Kerstein, 2002; Lyder, 2011) and may have a more complex aetiology than other anatomical areas of the body. These issues could be related to the anatomy of the area, with a thin layer of subcutaneous tissue covering the calcaneum, which is not served by a major artery, together with the influence of certain comorbidities. This leads to vulnerability to pressure injury and requires a preventative approach that understands that certain patient groups are very vulnerable and are at higher risk of pressure injury (Hampton, 2003; Walsh and Plonczynski, 2007; Donnelly et al, 2011; Young, 2017). These vulnerable patient groups also contribute to the highest cause of non-traumatic amputations. People with diabetes, renal failure and other complications that result in reduced/altered sensation about the lower limbs and/or lower-limb vascular status (e.g. vascular disease, stroke, HIV, advanced age, sensory deficit, spinal cord injury, immobility, obesity, poor nutrition) are at an increased risk of developing pressure ulceration on the heel (Blaszczyk et al, 1998; Hampton, 2003).
As demonstrated from the pressure ulcer classification guide (Figure 1), the early signs of pressure ulceration can be very subtle; therefore, knowing what signs to look for and having the ability to see this is crucial. Easy identification and monitoring of the heel in particularly vulnerable groups is essential.
Multiple clinical guidelines recommended the use of robust assessments to identify at-risk patients and the application of heel-protection devices to reduce the likelihood of developing heel pressure ulcers, with the incidence of heel pressure ulcers seen as being inversely correlated with the number of heel protectors used, and that the consistent and early use of heel protectors improved patient outcomes and reduced costs of care (Rajpaul and Acton, 2016). This finding was largely dependent on performing a structured risk assessment upon admission to an acute hospital, or as soon as feasible, in order to identify patients at risk of developing pressure-related skin breakdown. Following a risk assessment being conducted, risk-specific interventions should then be employed in order to reduce the risk of the development of pressure ulceration (European Pressure Ulcer Advisory Panel [EPUAP] et al, 2019), with daily reviews and reassessment when clinical indications are present (Cuddigan et al, 2008; Institute for Healthcare Improvement, 2011; Rajpaul and Acton, 2016) to allow any skin damage to be noted at an early stage.
In an oral presentation at the International Symposium on the Diabetic Foot in 2015, Gerry Rayman presented the results of a study using an assessment tool (Rayman et al, 2011; Sharma et al, 2014) to reduce the incidence of hospital-acquired foot ulcers in people with diabetes. Rayman et al (2015) compared the rates of foot pressure ulceration in inpatients with and without diabetes before and after the introduction of the tool. The authors reported that, following introduction of the tool, the rates of hospital-acquired foot pressure ulcers in people with diabetes fell by 60%. This was a greater fall than in those without diabetes, who saw a reduction of 44%.
Evidence-based education therefore needs to be provided to healthcare staff in order to improve the accuracy and performance of regular foot checks to allow for the recognition, prevention, treatment and management of heel pressure ulcers, and to reduce the risk of avoidable harm to patients.
Research has shown that effective offloading of the heel protects vulnerable heels from pressure damage (Junkin and Gray, 2009; Donnelly et al, 2011); therefore, the investment into appropriate offloading and protective devices as part of a comprehensive strategy for risk-stratified prevention of pressure ulcerations is essential (EPUAP et al, 2019). Evidence-based best practice for heel pressure ulcer prevention should be implemented as soon after the initial risk assessment is undertaken to ensure patient safety and improved outcomes (Lyder, 2011; EPUAP et al, 2019).
Evidence available suggests that a reduction of incidence in pressure ulcers results in improved patient outcomes, increased quality of care and greater cost efficiency (Rajpaul and Acton, 2016).
From liaison with clinically experienced nurses and other healthcare professionals within the NHS London Clinical Networks for Foot Care and Renal Network, the thought of having a handy guide of the protocols and any useful tool to assist in checking the feet was raised by many. Further discussions were then held with those clinicians performing foot checks, where the following was noted:
- Development of a practical tool and protocols are needed to improve full and comprehensive daily quality foot checks for people with known vulnerabilities for inpatients and for every clinical engagement for outpatients.
- Having a guide which people would carry in a pocket and would be expected to transfer between uniforms wasn’t considered helpful. There was a preference for something that would be available/on-hand and not something which is heavy, bulky or which they would need to take out of their pockets.
- Many valid concerns and issues were raised regarding health and safety, infection, prevention and control (IPC), and safe movement and handling in order to allow people to inspect the back of a person’s heels easily. Comments received include potential difficulties in: bending down to look around the foot; difficulties lifting a limb and bending down to look at the same time (especially if the leg is big/heavy); issues with getting the head/face close to/against the mattress or the floor; kneeling and leaning to see difficult-to-view areas; and problems lifting up a heavy limb and trying to look behind/underneath it.
Literature is available which advocates the use of mirrors in checking patients’ heels, which would address the issues raised regarding manual handling concerns when conducting a routine inspection of a patient (NHS England et al, 2013; Nursing Standard, 2012; Nursing Times, 2015; Advanced Tissue, 2015; Ousey et al, 2018; Stephens and Bartley, 2018). Unfortunately, IPC protocols prevent the use of standard mirrors on wards and within clinical environments if encased or within a hinged bracket, with health and safety concerns also being present in case of sharp edges or a standard mirror shattering.
Experiment
In order to appreciate the current effectiveness of foot checks being performed, a simple experiment was conducted to see how much of the foot can be seen easily, without having to adopt strenuous or risky positions. The concept was initially to determine whether people could see the whole area about the hindfoot and identify different patches.
A ruler was coloured in with different colours, not all of which were the same measurement, with three areas of demarcation included, which were meant to represent an area of demarcation and an immediate concern (highlighted within red circles in Figure 3).
Results
Nineteen of those who took part in this experiment (38%) looked at each side of the hindfoot and considered they were able to see all of the surface area of the heel, informing that they could see all of the colours.
- 31 of the participants (62%) stated that they could not see the back of the heels without having to adopt poor manual handling techniques or poor postures.
- 90% stated they could see the area of demarcation within the “pink zone”.
- 50% confirmed identifying the area of demarcation in the “yellow zone”.
- Nine participants (18%) thought the area of demarcation in the “yellow zone” to simply be a “smudge”.
Participants were then handed a mirror and asked to repeat their assessment (Figure 4). The mirror allowed for the whole of the foot to be seen, including an almost 3-cm area which people were not able to acknowledge before, with the area of demarcation being able to be identified. All of those taking a second attempt to check the foot with the mirror were able to notice this previously unseen area, with some commenting “I didn’t know there was a red bit or a purple area”, not to mention the other previously undetected area of demarcation. This small study highlighted the importance of accurate skin observation, the need to know what you are looking for and the use of appropriate equipment, such as mirrors.
Increasing education on the importance of daily, quality foot screening/checks and being able to do this process properly should help healthcare staff in the care and management of vulnerable patients, increasing awareness and improving the frequency and quality of foot checks. This should facilitate earlier identification and subsequent referrals and provision of protection when required, thereby reducing the number of avoidable pressure issues. Unfortunately, the use of mirrors within the majority of hospitals and clinics contravene IPC and health and safety protocols.
The Foot Check Card concept
From liaising with various members of the multidisciplinary healthcare services, work was undertaken to develop a practical tool which is associated with the existing foot check protocols in order to improve full and comprehensive daily quality foot checks for people with known vulnerabilities for inpatients and for every clinical engagement for outpatients.
There are many risk-assessment tools currently used in clinical practice to estimate the risk of developing a pressure sore, including, but not limited to, the Waterlow scale, the Braden scale, the Norton scale, the Glamorgan Pressure Injury Screening Tool and the pressure sore prevention score. All of these tools fail to educate on the specific issues/risks surrounding heel ulceration or to support an assessment of the foot to identify the presence of peripheral arterial disease or neuropathy, but rather focus on skin inspection.
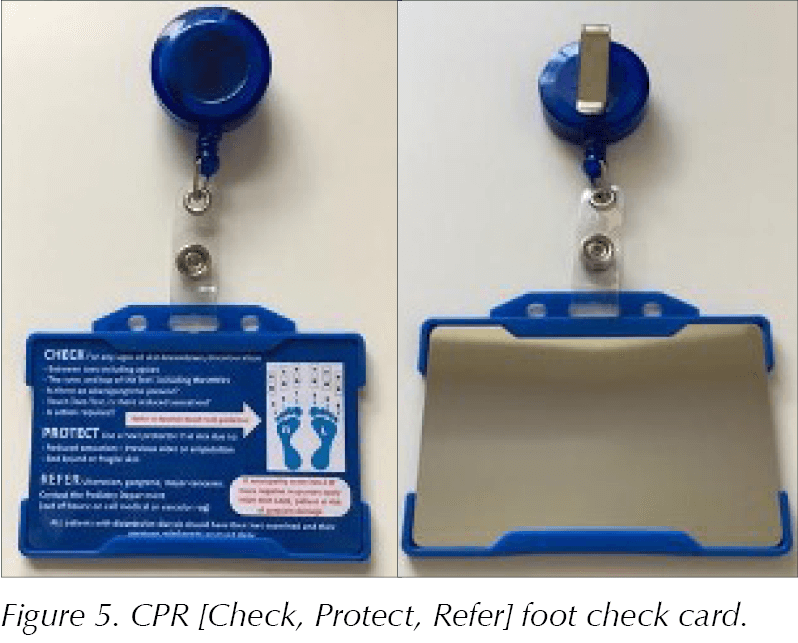
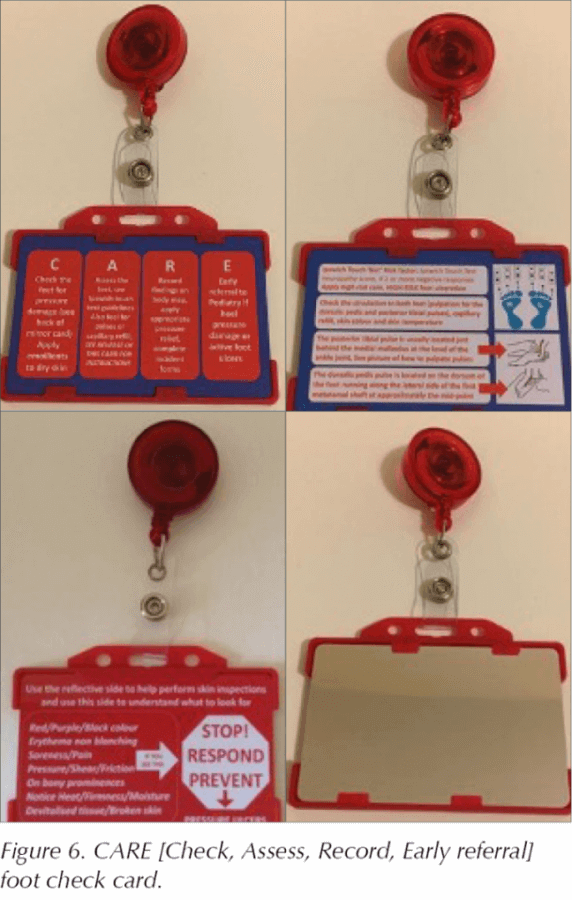
Work which the Scottish Diabetic Foot Action Group have put forward – the Check, Protect, Refer (CPR) protocol – and that of Cardiff and Vale University Health Board (the Check, Assess, Record, Early referral [CARE] protocol) had already been adopted by many Trusts, as well as some charities to help support the need for regular foot checks of vulnerable patients in order to reduce the number of pressure problems, wound/sore development, potential infection and amputation. The CPR and CARE processes are quick, simple and straightforward, without relying on any other tools to be used.
In conjunction with a risk assessment scale for pressure ulcer development and the SKIN (Surface, Keep moving, Incontinence, Nutrition) Bundle, the CPR and CARE protocols highlight that patients admitted to hospital with diabetes and other complications causing altered lower-limb sensation or vascular status are at a high risk of developing heel pressure damage.
A flexible, shatterproof, wipeable mirror with bevelled edges and fully compliant with all IPC and health and safety requirements was developed in order to aid healthcare professionals in looking behind the heels of vulnerable patients. The mirror also allows inspection of other difficult-to-assess/view places for pressure problems developing, such as bony prominences, identification of devitalised/discoloured tissue and broken skin. The mirror was made to be the same size as a standard NHS staff ID card (thereby allowing it to be held within a two-sided card holder) with CPR (Figure 6) protocol instructions and guidance printed on the reverse, allowing a staff ID to be held in the empty side of the card holder. This badge can attach to a retractable lanyard so that the person performing the simple foot checks doesn’t have to unclip it every time. The CARE protocol includes a second card, which has the mirrored surface on one side with indications of what to look for as indications for possible soft tissue breakdown.
The use of these cards and protocols would allow people to routinely review patients and their vulnerable feet easily, with reduced variation between practitioners, disciplines and level of experience. The information on the foot check cards and supporting information leaflets developed (one for healthcare professionals using the tool and one for patients) have been ratified and endorsed by recognised societies, professional bodies and various Trusts in order to ensure concordance with the information and direction given. The use of these cards and established protocols should reduce the degree of variation between healthcare professionals performing the foot check, and improve referral rates and patient care and safety.
The cards are long-lasting, so would not need to be replaced frequently, thereby being a good return on investment, with each Foot Check Card (complete with double card holder and retractable lanyard) costing £3, which is negligible when compared against the cost to treat a preventable pressure ulceration as calculated by Dealey et al (2012; Table 1). Each individual card is also available individually, thereby reducing the need to purchase the entire unit (i.e. lanyard and card holder) for replacement as required.
Due to high demand, a version of the Foot Check Card was designed for diabetic foot screening (Figure 7), which comprises two cards: one contains the directions required to perform a comprehensive foot screening protocol on one side, with the annual care processes on the reverse. The second card in the holder has the mirrored surface on one side, with the advice on what to look for regarding soft tissue breakdown on the reverse (as with the CARE card). This foot screening comes with an accompanying information leaflet to help determine levels of foot risk and directions of onward referral as required.
Magnets for use on wards
In addition to the mirrored foot check cards, magnets have been developed following discussions with inpatient staff to help improve awareness of those who have been identified as either vulnerable for the development of foot complications or requiring offloading (Figure 10).
Conclusion
Implementing the policy of daily foot checks for all inpatients with impaired/altered sensation and/or reduced vascular status, using the foot check cards and following either the CARE or CPR protocol, allows the simple, safe, effective, repeatable, reliable and cost-effective performance of foot checks and early detection of vulnerable patients. This should lead to a reduction in the number of avoidable heel pressure ulcers through systematic checks and early detection. This should in turn lead to reduced costs in treating foot ulcers and subsequent complications, and improved standards of nursing, along with reduced health-and-safety and manual-handling risks and improved results in local and national audits (such as the National Diabetic Inpatient Audit). Further benefits include:
- Improved foot health and wellbeing of patients by reducing the number of avoidable foot complications from tissue breakdown with regular, quality foot checks, early detection and provision of protection when in bed, and timely referrals as required, along with improved information being provided.
- For vulnerable patients, the reduced risk of tissue breakdown results in lower rates of pain, reduced mobility, local and systematic infections, renal and multi-organ failure, limb loss and death.
- For a hospital Trust, a reduction in avoidable heel sores and skin breakdown results in reduced costs to treat infection and provide rehabilitation following amputation/surgery, as well as reduced numbers of delayed discharges as a result of avoidable heel breakdowns and subsequent issues. This would also have a reputational advantage for the Trust and would show an investment in people (e.g. patient safety, supporting patients to avoid long hospital stays, health and safety and vulnerability of staff) and improved accountability and documentation to aid with audits (Trust-wide and national).
- For staff performing foot checks, there are improved health-and-safety and manual-handling techniques when performing foot checks, as well as reviews of other areas prone to tissue breakdown, with reduced sick days from assessing staff due to back issues brought on from poor posture and manual handling. There is also the improved ability to view hard-to-reach/see areas, with a guide as to what is recommended, thereby improving staff knowledge and reducing the variation in process and recording of information regardless of discipline or level of experience.
Following a thorough review of inpatient foot checks and protocols in Scotland, work has been carried out by a multidisciplinary panel of healthcare professionals to standardise the pressure-relieving/redistributing products that are used across Scotland, with the award of this contract going to TalarMade, which has resulted in the following:
- Ensured suitability of product.
- Ensured quality of product.
- Standardisation of use.
- Reduced cost.
- Availability of the chosen pressure-redistributing products through the Scottish National Distribution Centre.
With this consistency and standardisation ensured, training resources have been able to be produced: https://learn.nes.nhs.scot/3704/rrheal/healthy-aging/cpr-for-feet
Resources
The Mirror Foot Check Cards and magnets are available at: www.respond2pressure.co.uk or www.mirrorbadge.com, with accompanying ratified information leaflets available for the Mirror Foot Check Cards which can be personalised for individual Trusts.
For further details regarding the CPR protocol, please contact Duncan Stang, National Diabetes Foot Co-ordinator, Scottish Diabetes Foot Action Group,
on the following email address:
[email protected]
Publisher’s note: This article was co-published in this journal and The Diabetic Foot Journal.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nicola Milne discusses how care is shifting to a more proactive, prevention-focused model.
22 Jul 2026