
Type 2 diabetes is a progressive, long-term condition associated with increased morbidity and mortality. People with diabetes have to make multiple daily choices about the management of their condition, often with minimal input from healthcare professionals (Jarvis et al, 2010). The necessary lifestyle changes and complexities of management make education a central part of diabetes management. Structured education programmes can help adults with type 2 diabetes to gain the knowledge and skills needed to effectively self-manage their condition (NICE, 2011).
Nationwide programmes such as Diabetes Education and Management for Ongoing and Newly Diagnosed (DESMOND) and the X-PERT Diabetes Programme are available for people with type 2 diabetes (Khunti et al, 2012; Deakin and Whitham, 2013). However, many diabetes services have developed their own programmes based on the needs of the local population (Daley et al, 2006; Daley et al, 2008; Daley and Wallymahmed, 2014). Quality assurance of such programmes is important to ensure that people with diabetes are receiving optimal education. NICE (2015) states that any structured education programme for adults with type 2 diabetes should have the following attributes:
- Is evidence-based and suits the needs of the person.
- Has specific aims and learning objectives, and supports the person and their family members and carers in developing attitudes, beliefs, knowledge and skills to self-manage diabetes.
- Has a structured curriculum that is theory-driven, evidence-based and resource-effective; has supporting materials; and is written down.
- Is delivered by trained educators who have an understanding of educational theory appropriate to the age and needs of the person, and who are trained and competent to deliver the principles and content of the programme.
- Is quality-assured and reviewed by trained, competent, independent assessors who measure it against criteria that ensure consistency.
- Outcomes are audited regularly.
The challenge for providers is to seek assurance that the structured education programmes they are providing for people with diabetes are fit for purpose and NICE-compliant. Acquiring certification from the Quality Institute for Self Management Education and Training (QISMET) is a way of doing so.
What is QISMET?
QISMET is an independent body which has developed quality standards and certification for self-care management for a range of long-term conditions, including diabetes. The diabetes self-management education quality standard (QISMET, 2016) allows providers to demonstrate that they are meeting NICE (2011) criteria for structured education. There is a cost involved for certification, and this will vary according to the organisation seeking accreditation. In the authors’ case, this was was £2200 to assess two programmes delivered across six venues. According to its website, QISMET is not a profit-making organisation.
The certification process
The QISMET process involves seven steps:
- Initial contact – providers contact QISMET for information and advice.
- Application – the application form is completed and submitted. A quote is given and, if accepted, an invoice is sent.
- Self-assessment – an auditor is allocated once the invoice has been paid. The provider completes a self-assessment workbook to identify any outstanding issues. Once the provider considers that all the requirements of the quality standard are met, the completed workbook and other relevant documents are submitted to the auditor for a desktop review.
- Desktop review – the completed self-assessment workbook, along with other requested documents, are submitted and examined by the auditor. If they are complete and satisfactory, an audit visit date is agreed.
- Audit visit – during the visit, the auditor interviews key members of the provider team to ensure that the defined processes are being followed in practice, desired outcomes are being achieved, records are being kept and the programme is being effectively managed and implemented. It is expected that this will take at least one day.
- Follow-up – a report is provided by the auditor with a recommendation for either immediate certification or detailing any improvements that might be needed, with a deadline for the improvements to be in place. The provider submits evidence to the auditor about the improvements undertaken and the auditor considers whether they are effective. If so, certification is recommended.
- Certification – moderation of the report and recommendation is undertaken by QISMET, and formal certification is granted. A certificate is issued, a logo provided and the provider is put on the certification register on the QISMET website.
Further details of the QISMET process, including the quality standard which informs the self-assessment (QISMET, 2016), can be found on the QISMET website at: http://www.qismet.org.uk.
The Sefton experience
Sefton is a borough in the North West of England which is divided into two Clinical Commissioning Groups (CCGs): South Sefton CCG and Southport and Formby CCG. The total population is approximately 279 256 residents (154 732 in South Sefton and 124 524 in Southport and Formby). Both CCGs have a significantly higher proportion of residents over the age of 65 years (19% in South Sefton and 25.4% in Southport and Formby) compared with the national average of 17.3% (South Sefton CCG, 2018; Southport and Formby CCG, 2018). Diabetes prevalence rates are 7.0% and 7.2%, respectively.
South Sefton CCG takes the lead for commissioning structured diabetes education, which is delivered by two local providers, Mersey Care NHS Foundation Trust and Lancashire Care NHS Foundation Trust. Both providers have a strong history of delivering structured education and have worked together (and with other local Trusts) to develop two structured diabetes education programmes:
- Diabetes and You is a two-session (half-days), multidisciplinary education programme for people with newly diagnosed diabetes. This programme has been up and running for many years and was developed with the needs of the local population in mind.
- Diabetes and More is a two-session (half-days), multidisciplinary education programme for those with established diabetes that aims to reinforce and build on existing knowledge. This programme has only been introduced over the past 12 months.
The content of the programmes delivered by the two providers is essentially the same, with minor amendments to meet local needs. In 2017, South Sefton received NHS transformation funding to further develop the structured education programmes. QISMET accreditation was an expectation of this funding.
Self-assessment for QISMET certification
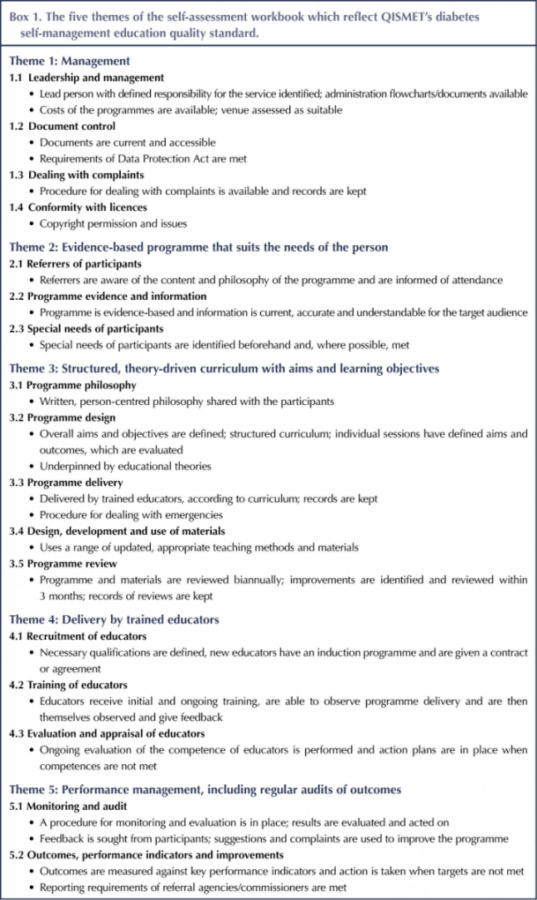
The QISMET accreditation process was coordinated by a diabetes project lead (MW); however, all members of the multidisciplinary structured education team worked together to provide evidence for the five themes included in the self-assessment workbook (see Box 1). This workbook, along with additional information documenting the organisational structure and details of the specific programme(s) for certification, forms the basis of the auditors’ desktop review. Providers are asked for specific evidence in support of every element of each theme. There may be one or two areas that providers are unable to meet completely before submission. However, if there is a plan to meet this requirement, the auditors may take this into consideration. For example, Sefton was unable to provide current costings before submission; however, these details were available on the day of the audit.
The self-assessment documentation can appear a little daunting to begin with. However, information in support of each of the requirements is really a reflection of what a structured education programme should be doing. If providers are unable to give evidence for a specific requirement then this should be viewed as an opportunity to improve the quality of the programme. A timeline of goals to achieve the requirements should be set, with regular review. However, the self-assessment workbook should not be submitted until the providers are able to demonstrate compliance with the requirements before the audit date. At Sefton, some time was spent reviewing the learning outcomes for each session to ensure that they were measurable and reflected in the session plans.
It is important to remember that some members of the structured education team, particularly newer members, may not be au fait with QISMET. Time should be taken to meet with the team to ensure they are all aware of what QISMET is, the benefits of accreditation and their role in achieving this.
Audit visit
Prior to the audit visit, the auditor provides a list of staff members to be interviewed. Face-to-face interviews are preferable but this is not always possible for all staff concerned, and at Sefton one member of staff was on a non-medical prescribing course, so arrangements were made for her to be interviewed by phone. The auditor was provided with a paper-based file containing all of the documents included in the self-assessment workbook to refer to during the audit visit. This is a live document which is now updated on a regular basis if any changes to the programme or the staff delivering it are made.
Some staff members were anxious about the interviews as they did not know what to expect. However, the Sefton experience was that the auditor wanted to ensure that we were doing “what we said on the tin”. Interviews are relaxed; the auditor is not there to catch anyone out, and in fact they can provide very useful feedback. At the end of the day, the auditor gives verbal feedback to the structured education lead. This is then followed up by a formal report highlighting strengths and possible improvements, and comments from the providers are encouraged. If all standards are met, accreditation is recommended and a certificate issued.
Benefits and challenges
The QISMET accreditation process and certification has many benefits, including the following:
- Allows providers to critically review their structured education programmes and make necessary changes to improve the quality of the programme.
- Ensures that the views of participants are considered.
- Reassures providers that structured education programmes are meeting NICE (2011) guidance.
- Reassures commissioners that structured education programmes are meeting NICE requirements and have been assessed by an independent body. This may be a prerequisite for commissioning structured education programmes in the future.
- Providers will have a live, dynamic portfolio of evidence which can be updated as needed. This will form the basis for reaccreditation in 3 years.
- An acknowledgment of the hard work, time and effort that the structured education team has put into developing and reviewing the programme.
There will of course always be challenges. It is likely that providers will need to make some changes or additions to achieve QISMET certification. These may be relatively easy to implement, such as ensuring that all of the venues have a current venue assessment. More challenging issues may be, for example, developing a robust training programme for new educators. Other local providers should be able to offer some advice. Some providers may be developing new programmes, and the QISMET process can serve as a guide to what is required to deliver a quality service.
Time is always a challenge for this important yet not necessarily urgent adjunct to a service. Assigning a specific person to coordinate the process is essential, but everyone should have their own responsibilities. It is useful to develop a timeline, plan regular reviews and, if possible, try to allocate protected time.
Conclusion
It is important to highlight that QISMET certification is not a paper exercise. Sefton already had an established, dynamic structured education programme (Daley and Wallymahmed, 2014); nevertheless, areas for improvement were identified during the QISMET process. The two providers engaged, worked together and reported a worthwhile and bonding experience. Since achieving QISMET certification, the team has been working with the local Improving Access to Psychological Therapies team and has agreed to include this in the programme. Finally, following certification, take the opportunity to publicise and celebrate your success – you deserve it!
Acknowledgement
Thanks are due to all members of the Mersey Care NHS Foundation Trust and Lancashire Care NHS Foundation Trust multidisciplinary structured diabetes education team.




Developments that will impact your practice.
7 May 2025