

Gestational diabetes (GDM) is a form of diabetes that occurs only during pregnancy. In the past two decades, GDM rates have increased dramatically (Carolan et al, 2012). In the US, Hispanic women from disadvantaged backgrounds are most at risk of developing this condition and having it mismanaged. This can have an effect on the health of both the mother and the infant.
Problem statement
The Centers for Disease Control and Prevention (2021) state that every year 2–10% of pregnant women will develop GDM within the US. If left untreated, women who have GDM are at increased risk of developing high blood pressure and pre-eclampsia during pregnancy (Carolan et al, 2012). Furthermore, women who develop GDM have a 50% greater risk of developing type 2 diabetes than those who do not, and Hispanic women have a more than doubled risk of developing type 2 diabetes compared with non-Hispanic white women (Bower et al, 2019).
The US Preventive Services Task Force (2021) recommends that pregnant women be screened for GDM between 24 and 28 weeks’ gestation. To help manage GDM, patients should be instructed on appropriate diet, exercise/staying active, blood glucose monitoring and monitoring of the baby’s development. Some women will have to treat their GDM with medications such as metformin or insulin. In one study, exercise and dietary modifications led to an improvement in glycaemic control (Mpondo et al, 2015). Individuals who were not able to manage their condition with diet and exercise required pharmacological management.
Some pregnant women are not able to participate in this comprehensive care plan for GDM due to barriers and lack of access to care. Therefore, the purpose of this systematic review was to explore barriers to GDM screening and management, and their effects on patient outcomes in Hispanic women.
Methods
Eligibility criteria
Studies on screening, management and barriers to treatment for GDM were included. Studies were included if any women reported factors that facilitate or inhibit GDM management. Additional inclusion criteria included studies conducted within the US or Australia, written in English, between the years of 2010 and 2020. Qualitative studies were considered and different research designs were utilised.
Search strategy
The electronic resource databases used were CINAHL, Medline, PubMed, EBSCOhost, and Google Scholar. The following key search terms were used: gestational diabetes, screening, management and barriers. BOOLEAN search included: gestational diabetes OR gdm OR diabetes in pregnancy, AND barriers OR obstacles OR challenges OR difficulties OR issues OR problems OR limitations, AND women OR females, AND Hispanic OR Latino OR Latina OR Mexican OR Central American OR South American OR Hispanics OR Latinos.
Selection process
The selection process was according to PRISMA guidelines. The author read each article’s title and abstract and applied the inclusion criteria. Once reviewed, the author retrieved the full-text article and the final decision was based on the inclusion criteria, analysis of Hispanic women and the purpose of the systematic review.
Quality assessment
Levels of evidence were determined according to American Association of Critical Care Nurses (AACN) criteria. The AACN evaluates research on two levels, to include grading the evidence using a system of levels and individually critiquing the research (Peterson et al, 2014). The purpose of determining the levels of evidence and grading of the evidence is to help with evaluating the credibility, reliability and validity of the research.
Another appraisal tool used for quality assessment was the Joanna Briggs Institute (JBI, 2021) Critical Appraisal Tool for Qualitative Research.
Data extraction and synthesis
Data were extracted from each study using the subheadings: author (year), study aim, design of study, participant demographics and concluding points. Data were extracted to depict the sample representation of Hispanic women with GDM along with findings related to the objective of this systematic review.
Results
Search results
In total, 38 articles were identified through Medline, 37 through CINAHL and 37 through PubMed. After exclusion of fifteen duplicates, 97 articles were identified and reviewed based on their title, abstract and eligibility criteria. This yielded four studies to be used within this systematic review.
Study characteristics
All four articles were qualitative studies and all were published between 2012 and 2020. All four studies performed small focus groups with peer-to-peer interviews; one study also allowed participants to do telephone interviews. All four groups were audio recorded. The study participants were Hispanic women aged 18–45 years with a diagnosis of GDM. Two studies were conducted in Ohio, one in Chicago and one in Melbourne.
Quality assessment
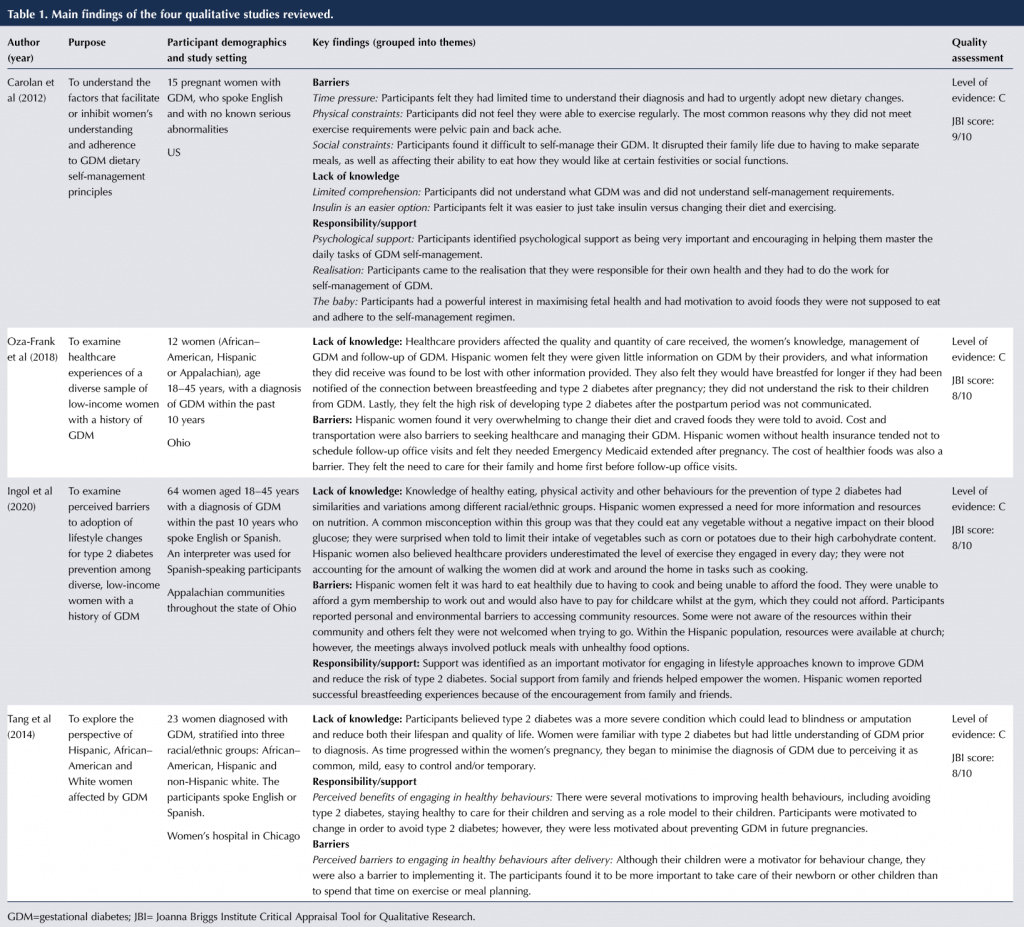
The quality assessment for each article was evaluated using the JBI tool for qualitative studies. Quality assessment for each study is described within Table 1. Oza-Frank et al (2018), Ingol et al (2020) and Tang et al (2015) scored 8 out of 10 on the tool and Carolan et al (2012) scored 9 out of 10; these high scores indicate that the articles were effective to use within a systematic review. The level of evidence for each study, according to AACN criteria, was ranked as C, which indicates there is not enough evidence to recommend for or against the inclusion of the condition in a periodic health examination.
There was low risk of bias due to the satisfactory selection of the target group to include Hispanic women aged 18–45 years with a diagnosis of GDM. Each study also had English- and Spanish-speaking participants. However, one study recruited women with a history of GDM within the past ten years, which may have introduced recall bias if the participants found it difficult to recall their experience, as well as potentially making the study less relevant to current practice. In another study, there was potential bias because most of the participants were highly educated and were self-selected; those who opted out may have had greater knowledge about GDM and more motivation to improve their health, in addition to facing fewer barriers to behaviour change and healthcare access.
Findings
The principal findings of the four studies are presented in Table 1. The studies identified a number of factors that either assisted or made it difficult for Hispanic women to screen and manage their GDM. Three themes were identified: barriers; lack of knowledge; and responsibility and support. Within the theme of barriers, three subthemes also emerged: (1) time pressure, (2) social constraints and (3) physical constraints.
Barriers: Time pressures
Hispanic women found time pressure to be a barrier due to not having enough time in the day to manage their GDM alongside their work and their families. They found it more important to take care of their family and homes: tasks such as working, cooking, cleaning and taking care of their children. Another time pressure that was discussed in one study was insufficient time to understand their diagnosis and urgently adopt new dietary changes (Carolan et al, 2012).
Barriers: Social constraints
The second subtheme explores social constraints. Hispanic women found it difficult to afford certain food options and found themselves cooking two different meals for their family and themselves. They also had transportation issues and were sometimes unable to come to follow-up office visits. Participants in one study did not have health insurance and were not able to follow up in the office (Oza-Frank et al, 2018). They felt they needed Emergency Medicaid extended after their pregnancy to continue to follow up on their management and make sure they had not developed type 2 diabetes.
Participants were also unable to afford a gym membership to work out and would not be able to pay for childcare whilst at the gym (Ingol et al, 2020). Some participants were not aware of resources available within their community, and those who were did not feel welcome when trying to attend.
Barriers: Physical constraints
The third subtheme explores physical constraints. Participants did not feel they were able to exercise regularly as advised by their healthcare provider or diabetes educator. The most common reason for this was pain: most participants stated they had pain in their pelvis or back and were unable to exercise or move a great extent due to this (Carolan et al, 2012).
Lack of knowledge
Lack of knowledge was a barrier to the screening and management of GDM. In all four studies, Hispanic women felt they did not fully understand what GDM was, nor did they understand the requirements for self-management with diet, exercise and blood glucose checks. They also felt they were given little information on GDM by their healthcare provider. In one study, they were unaware of the high risk of developing type 2 diabetes postpartum (Oza-Frank et al, 2018). However, in another study, participants believed type 2 diabetes was a more severe condition which could lead to blindness, amputation and reductions in life span and quality of life (Tang et al, 2014). This lack of understanding of GDM led participants to minimise their diagnosis and perceive it as common, mild, easy to control and temporary.
In one study, there was a misconception of what foods participants should eat, and they were not given examples of what to eat (Ingol et al, 2020). There was also a misconception on exercise; participants felt as though healthcare providers underestimated the level of exercise they engaged in every day, and that the walking done at home and at work was not counted as exercise (Ingol et al, 2020). In another study, participants felt it was easier to take insulin than to change their diet and exercise (Carolan et al, 2012).
Responsibility and support
Participants identified support as being an important motivator to help them engage in lifestyle changes such as diet and exercise. Support from family and friends also helped to empower them. Through the support of family and friends, participants engaged in lifestyle changes and stayed motivated for their children and family, and this helped them to avoid developing type 2 diabetes postpartum (Tang et al, 2014). With support from family and friends, participants also realised they were responsible for their own health and had to do the work to self-manage their GDM (Carolan et al, 2012).
Implications for practice and future research
This study has important implications for practice because every year 2–10% of pregnant women will develop GDM. If left untreated, these women have a higher risk of developing type 2 diabetes after delivery. Therefore, it is important to address the three themes that were identified within this study. It is imperative to provide Hispanic women with education, resources and the tools they need to self-manage their GDM. These women should be given information on GDM and examples of how to manage it through diet, exercise and potentially medication. Resources such as diabetes education classes should be provided to these individuals.
Successful self-management of GDM is associated with lower rates of serious pregnancy complications, infant morbidity and risk of developing type 2 diabetes later in life (Carolan et al, 2012). It is also important to continue to encourage Hispanic women to utilise their support system of family and friends, who can motivate and encourage them with their lifestyle changes, as well as help them recognise that they are ultimately responsible for their own health.
Study limitations
One limitation of this systematic review is that the research yielded only four studies for analysis, all qualitative studies. Other study designs with statistical analysis could have been used to explore the data further and make the systematic review more in-depth. Even though all of the studies used in this analysis were qualitative studies, they all ranked either an eight or nine out of ten on the JBI Critical Appraisal Tool, which helps evaluate the credibility, reliability and validity of research (Peterson et al, 2014).
Conclusions
In conclusion, this study indicates that Hispanic women aged 18–45 years with a diagnosis of GDM often have barriers, lack of knowledge and need for support/responsibility in the self-management of the condition. They require supportive services to help with the self-management of GDM and improve their outcomes.



Developments that will impact your practice.
25 Jun 2026