

It is expected that diabetes specialist nurses (DSNs) hold the Independent Prescribing qualification, and that those new to the speciality should develop their knowledge and competence with a view to attaining it (Trend Diabetes, 2024). Whilst this approach is considered best practice, a supportive framework is needed to enable the non-prescribing DSN to practise actively within the service as they develop the appropriate knowledge and skills to undertake the Independent Prescribing qualification. This article describes the process undertaken in our community Trust to establish such a framework.
Independent prescribing
Independent prescribing is now a well-established aspect of specialist clinical practice, aligning with NHS principles and drivers to address the increasing complexities in patient care and the demands on the health service. Dunn and Pryor (2023) state that independent prescribing has developed significantly and will need to continue to do so as nursing roles and education change to meet evolving population health needs. Prescribing practice is governed by ethical and legal principles to ensure a holistic patient-centred approach (Royal Pharmaceutical Society [RPS], 2021). It has been recognised as a valuable resource that can reduce hospital admissions and long stays, and improve quality of life for those with long-term conditions and multimorbidity. The initial focus of Government policy regarding non-medical prescribing was on improving patient access to medicines (Graham-Clarke et al, 2019).
Qualified independent prescribers (IPs) can assess, diagnose and prescribe any licensed medicine and products listed in the British National Formulary (BNF, 2024), provided this is within the area of their competence (Mitchell and Pearce, 2021; Royal College of Nursing [RCN], 2025a). They must have completed an Independent Prescribing course recognised by the Nursing and Midwifery Council [NMC].
Role of the DSN
The complications of diabetes are well established and may involve long-term damage, dysfunction or failure of various organs alongside the progressive development of micro- and macrovascular disease. Effective control of blood glucose levels influences the onset and severity of these complications. Appropriate adjustment and optimisation of diabetes medication is fundamental in achieving this (NICE, 2022a; 2022b).
DSNs work exclusively in diabetes management, and their role is integral within the multidisciplinary diabetes team. The value of the role is well recognised (Department of Health, 2012; Diabetes UK, 2019a). The role of the DSN centres on the assessment and monitoring of people with complex needs to ensure appropriate prescribing, dose adjustment and correct use of diabetes-related medications. However, a survey of diabetes inpatient specialist nurses (DISNs) reported that 49% were not prescribers and 9% expressed concerns that local guidance was needed to help them practice effectively (Lake et al, 2024). Many participants expressed uncertainty about what they were allowed to do as non-prescribers.
This theme is echoed in the Diabetes Specialist Nurse Forum UK. In this social media group, a common question is, “Has anyone got a policy to cover insulin titration by DSNs who aren’t prescribers?” Such posts attract many responses agreeing that the situation is ambiguous. Members often include offers to share locally developed approaches, which focus on titration by limiting or predefining oral and injectable dose adjustments, and require the non-prescribing nurse to use words such as “suggest” or “advise” when making such recommendations to the prescriber to enable a change in prescription. Ultimately, this approach leaves the prescriber to make the formal decision about altering the prescription, and does not give them assurance regarding the DSN’s competence to make such recommendations.
Case example illustrating challenges
This issue became evident when a GP was asked by a non-prescribing DSN to adjust insulin doses on a medication administration record. The GP questioned why this was not actioned by the nurse themselves or within the specialist diabetes team, having assumed that all DSNs were prescribers. The GP was confused about why there was a request to prescribe the medication.
Implications for prescribing practice
Independent prescribing enhances patient care by supporting timely access to medicines and enabling choice, whilst helping to reduce waiting times and hospital admissions, and maximising the wider skills of the healthcare team (NHS England, 2025). On reviewing this position with IPs in services across our Trust, there was consensus that IPs are not to prescribe for a patient they have not fully assessed themselves, even with a recommendation from a non-prescribing nurse. The preferred process appeared to be that recommendations for treatment changes should be sent to the GP for them to action the prescription.
Reflectively, this raised the question of why it is considered acceptable to ask a GP to make a prescribing change, but not a prescribing colleague within the team. No one could answer. This process risks delaying the patient’s access to the optimised treatment regimen and may confuse the GP who has referred the patient for specialist review of their condition and treatment, only to be asked to issue the prescription themselves.
The evolving role and competencies of DSNs
It is essential, therefore, that Band 7 DSNs hold (or are working towards) IP status (Diabetes UK, 2019b). This should be achieved by following nationally accredited competency frameworks, such as those from Trend Diabetes (2024) and the RPS (2021). Within the NHS, staff are paid according to a pay scale known as Agenda for Change (NHS Employers, 2026). Newly registered nurses join at Band 5, while nurse consultants are Band 8a and above.
Diabetes UK (2019a) has highlighted that, because there is no standardisation of the qualifications required to gain the title of DSN, it can be difficult to determine how “specialist” the diabetes nurse actually is. The DSN role, like many specialist nurse roles, requires a broad skill set aligned to the four pillars of nursing practice: leadership and management, education, research, and enhanced/advanced clinical practice (RCN, 2024b).
Currently, those joining a specialist diabetes nursing team may begin referring to themselves as a “diabetes nurse”. This creates inconsistencies in banding, skills and knowledge across DSN posts for the nurse who may be a specialist but is not an IP.
Training pathway development
To support nurses joining the diabetes team to progress towards becoming prescribers, a training pathway was developed. In addition to identifying the internal and external courses that new nurses would need to attend, appropriate shadowing opportunities were identified. This pathway empowers nurses to start building their confidence around prescribing prior to undertaking formal training, ensuring they are better prepared for the role.
By enabling a competent, non-prescribing DSN to make timely recommendations on medication management to IP colleagues, access to medications can be expedited, improving the patient experience. Previously, contacting the GP with information so that the prescription could be provided often led to delays in patients receiving updated medications, which could negatively affect outcomes and overall experience.
Trend Diabetes (2024) suggests that up-to-date and proficient DSNs have improved job satisfaction and enhance many aspects of service delivery, including safety, preventing harm and providing a positive experience. In addition to supporting nurses to develop the knowledge and skills required for the role, it is hoped that the pathway will also support recruitment and retention of nurses within diabetes teams, as nurses can see a clear way toward becoming a specialist nurse and advancing their careers.
A literature review by Armstrong (2023) identified positives for both nurses – such as increased job satisfaction, autonomy and responsibility – and for patients, including better outcomes, easier access to medication and higher overall satisfaction. However, the review also highlighted an ongoing need for support and professional development for nurses working as IPs.
Despite these benefits, this did not address the immediate need for a practical solution to ensure that service efficiency is maintained when patients are seen by non-prescribers.
Can a non-prescribing nurse complete an assessment and ask an IP to prescribe based on their recommendation?
The NMC and RCN were contacted for their positions on this type of practice. Their responses were that it remains the professional responsibility of the person issuing the prescription to ensure that prescribing is done safely. If an IP delegates the assessment of a patient’s suitability for a medicine, they must be satisfied that the person they delegate to has the qualifications, experience, knowledge and skills to make the assessment.
The General Medical Council (GMC, 2021) advises that if a prescriber prescribes on the recommendation of another health professional, they must be satisfied that the prescription is needed, is appropriate for the patient and is within the limits of the prescriber’s competence. Therefore, the guidance that is being shared in social media DSN networks is not in line with guidance from the NMC and RCN.
Enabling IPs to act on non‑prescriber recommendations
With the RCN and NMC advice in mind, the expected competencies for the non-prescribing DSNs were identified, and a pro forma developed to support the relay of appropriate information to the IP, enabling them to make an informed prescribing decision.
A standard operating procedure (SOP) was developed for our organisation to provide a supportive framework for both the IP and the non-prescribing DSN. It incorporates national guidance from the NMC (2018), RCN (2025a), GMC (2021) and RPS and RCN (2023) on how current working practice can be safely supported when prescribing changes are required but the specialist clinician is not an IP.
The SOP also sets out the responsibilities of the IP and the accountability of the non-prescriber. It aims to provide safe, consistent and professional standards for IPs to follow when prescribing at the recommendation of a non-prescribing DSN, for both oral and injectable diabetes medications aimed at improving glycaemic control. It includes guidance on the training, monitoring requirements and competency framework needed to support staff in delivering this service.
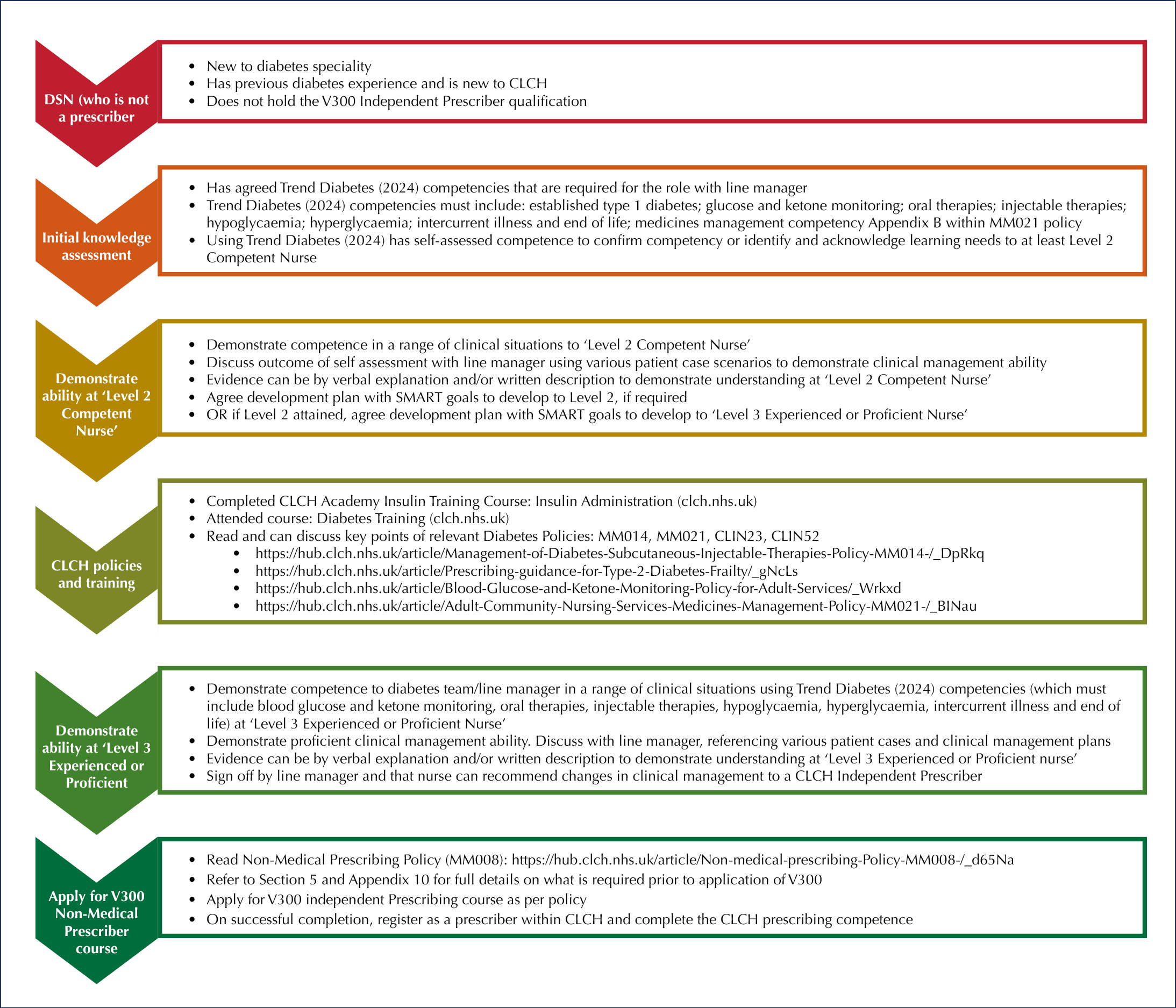
Competence is determined through observation and a verbal assessment of knowledge and skills. An overview of the process for the development of competence is presented in Figure 1. DSNs must be assessed and signed off as competent prior to making recommendations. This framework seeks to ensure that IPs and non-prescribing DSNs can work effectively together to make safe, appropriate medicinal changes for patients in a timely and efficient manner. It is to be used as an interim operational procedure to support safe care while DSNs transition from novice level to attaining the Independent Prescribing qualification.
Conclusion
The initial focus of Government policy on non-medical prescribing was to improve patient access to medicines (Graham-Clarke et al, 2019). With the development of this SOP, we have provided a mechanism to ensure that prescribers can be assured of the clinical competence of non-prescribing colleagues who make recommendations.
The SOP has received positive feedback, particularly regarding the clarity of the process for attaining competence. Patients are experiencing shorter waits for medication adjustments or initiation, which has improved efficiency. An audit of the non-prescribers’ documentation demonstrated a high standard of documentation and effective communication between non-prescribers and IPs.
Two areas for improvement were identified: firstly, the consistent documentation of allergies or recording “none known” where applicable; and secondly, letters to GPs or other external colleagues should stating that the nurse is a non-prescriber. These points will be discussed within individual clinical supervision sessions, and further refinements may arise from these discussions.
There is now interest from other specialist areas within the organisation in adopting the broad principles of this approach to support their staff to progressing to become Independent Prescribers.



EDENT1FI programme achieves landmark in early detection of type 1 diabetes in children.
17 Mar 2026