
Recent figures from Public Health England (PHE, 2018) have highlighted the significant levels of childhood obesity in England. The latest data from the National Child Measurement Programme indicates that 22.2% of Reception-aged children are overweight, with 9.3% of those being obese. By Year 6 (ages 10–11), this increases to 33.9%, with 19.6% being obese. Worryingly, the 2015/16 National Paediatric Diabetes Audit indicated that the prevalence of obesity in young people with type 1 diabetes is increasing and, in some age groups, demonstrated higher levels of obesity than in the general paediatric population (Royal College of Paediatrics and Child Health, 2017a; 2017b). In an attempt to tackle the issue of childhood obesity, the Government has produced a childhood obesity plan (HM Government, 2016), with the aim of significantly reducing England’s rate of childhood obesity within the next 10 years.
One aspect of the childhood obesity plan is the so-called “sugar tax”, or soft drinks industry levy, which came into effect in April 2018. The Government is also challenging all sectors of the food and drink industry to reduce sugar by at least 20% by the year 2020, across a range of products that contribute to children’s sugar intake. These include breakfast cereals, yoghurts, biscuits, cakes, sweets, morning goods, puddings, ice cream and sweet spreads.
Another aspect of the childhood obesity plan is “helping all children to enjoy an hour of physical activity every day” (HM Government, 2016). UK Physical Activity Guidelines (HM Government, 2011) recommend that children and young people should do 60 minutes of moderate to vigorous activity each day, including bone- and muscle-strengthening activities on three days of the week.
Physical activity is associated with beneficial effects for children in terms of body fat, cardiovascular risk, metabolic risk, bone health and psychological wellbeing (Department of Health, 2010; 2011). For young people with diabetes, physical activity is of particular importance because of the marked increase in risk of cardiovascular disease in this population. NICE (2015) guidance suggests that exercise should be encouraged on a regular basis in young people with diabetes to reduce the risk of developing cardiovascular disease. Additionally, some studies have found that physical activity can benefit overall glycaemic control. A meta-analysis by MacMillan et al (2014) found that exercise had a significant beneficial effect on HbA1c, with a weighted mean difference of –9 mmol/mol (–0.85%).
However, although the benefits of physical activity are significant, there are many perceived barriers for people with diabetes. For young people with type 1 diabetes, undertaking physical activity poses additional challenges for blood glucose management. Worries around loss of control of diabetes, fear of hypoglycaemia and, in older children, low fitness levels have been found to be barriers among young people and their parents (Jabbour et al, 2016).
It is essential that paediatric diabetes multidisciplinary teams encourage and facilitate physical activity in young people through the provision of evidence-based advice for glucose management. Individualising advice based on blood glucose results around physical activity is crucial for minimising barriers to exercise.
Identifying the need for guidance in local leisure facilities
In the local area of St Helens, the levels of overweight and obesity are above the national average, with 37% of Year 6 children overweight and 22% obese (PHE, 2018). This is echoed in audit data in the local paediatric diabetes population, where there is an even higher prevalence of obesity: 25.5% (RCPCH, 2017b). For this reason, there is a strong focus on the messages of healthy eating and a minimum of 60 minutes’ physical activity per day within the multidisciplinary team.
Several of the local Council-run gyms and leisure facilities offer membership for young people at a reduced price. However, when one of our patients attempted to access local gym facilities in an effort to improve their fitness for team sports, we were disappointed that their experience was negative and they were considering cancelling their membership to the gym. This was in part due to their initial difficulties accessing the gym on the grounds of having diabetes. Subsequently, they found that the guidance the gym followed for people with diabetes was so restrictive that exercise sessions were cut short unnecessarily. There was also a lack of understanding around the technology the young person used to manage their diabetes (insulin pump and continuous blood glucose monitoring). These were posing additional, external barriers to exercise for this young person.
Upon hearing of these difficulties, the diabetes team was keen to improve access for this young person in addition to other young people under its care. The local leisure facilities were contacted and offered training, specifically about supporting young people with type 1 diabetes. The staff were extremely keen for this to go ahead, and staff from all the local Council-run gyms attended the training.
Development and dissemination of the guidelines
The local gym staff had been previously been trained and provided with guidance in 2009 from the Wright Foundation CIC. Whilst this training provided a good foundation, it was neither recent nor specific to paediatrics. It therefore did not include some of the more recent evidence and did not acknowledge some of the newer technologies available in diabetes care.
Patients in our clinic are routinely counselled about exercise management during clinics and group education sessions. This involves guidance around the periods before, during and after physical activity has taken place. In contrast, the gym staff only needed guidance for the period of time in which the young person is in the leisure centre. Therefore, it was requisite that the guidance we developed promoted safety during the period immediately before the exercise, during the exercise and immediately after the exercise.
The training package was delivered jointly by the dietitian and paediatric diabetes specialist nurse in a meeting room at one of the local gyms. It incorporated education on the following subjects:
- The importance of physical activity for health in young people with diabetes.
- The successes of athletes with type 1 diabetes (including recent news stories regarding Diathlete and the Team Novo Nordisk cycling team). This was to demonstrate that type 1 diabetes should not be a barrier to exercise or performance.
- What type 1 diabetes is and the difference between type 1 and type 2 diabetes.
- Basic physiology around carbohydrates, insulin and blood glucose.
- A brief introduction to insulin treatments and technologies.
- How different types of exercise usually affect blood glucose (aerobic and anaerobic).
- Education around the guidelines, including pre-exercise targets and actions, during-exercise actions and general information around exercising with diabetes.
- Hypoglycaemia symptoms and treatment.
Pre-exercise guidance
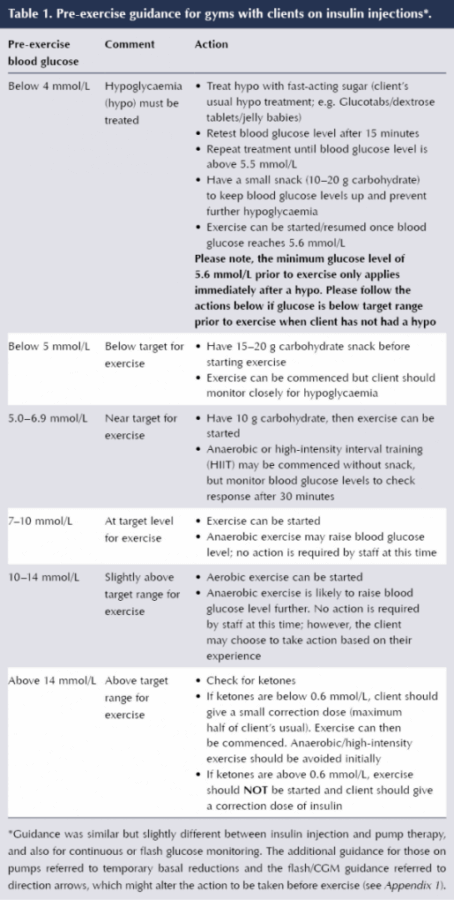
The guidance for actions based on pre-exercise blood glucose levels and during exercise was based on consensus guidance (Robertson et al, 2014; Riddell et al, 2017; NICE 2015). Much of the evidence that informed these guidelines is based on research in adults with type 1 diabetes. It was emphasised during delivery of the training that these are general guidelines and that individual plans may be provided by the diabetes team for young people based on their responses to the new exercise routines they will be undertaking.
The guidance for actions based on pre-exercise blood glucose levels are outlined in Table 1. These were less restrictive than the levels the gym staff had previously been recommending, which disallowed exercise if blood glucose was either high or below 6 mmol/L, or if it reached these levels at any point during the exercise. This had led to the individual with diabetes spending more time being unable to exercise than being allowed to. For this reason, as part of the training package and written guidance, we also delivered education on the expected effects of different types of exercise (including aerobic, anaerobic and mixed) on blood glucose levels.
For those young people wearing continuous glucose monitoring and flash glucose monitoring devices, specific guidance was developed. These contained caveats for actions depending on the direction of trend arrows (see Appendix 1).
During-exercise guidance
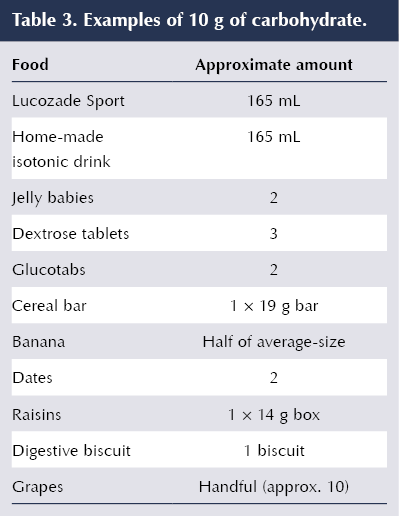
Guidance for young people regarding additional carbohydrate requirements during exercise recommends up to 1.0–1.5 g of carbohydrate per kg of bodyweight per hour during peak insulin action, with a lower requirement the further from the last bolus that the exercise is undertaken (Robertson et al, 2014). The actual amount of carbohydrate required during exercise is dependent on the type, intensity and duration of the exercise, in addition to the child’s weight (Riddell et al, 1999; Riddell and Iscoe, 2006). However, this advice was simplified for the gym staff to 30–60 g of carbohydrate based on the approximate weights of the young people in the age range currently allowed access to the gym (see the guidance in Table 2). Examples of what 10 g of carbohydrate looks like were provided (Table 3).

Written guidance was also provided about the symptoms and treatment of hypoglycaemia, and education was included in the training we provided.
General guidance
Some general guidance regarding exercising with diabetes was provided (Box 1), as the gym’s previous guidance was very restrictive about the time of day the person could exercise. For example, the previous advice suggested that exercise could not take place within 3 hours of bedtime and must be scheduled at the same time every day. This was impractical considering the usual routines of young people, with physical activity often taking place after school. Although we acknowledged that risk of nocturnal hypoglycaemia has been found to increase with exercise performed in the afternoon (Tsalikian et al, 2005; Gomez et al, 2015), we did not want to place further barriers to the young people exercising. This risk is something that is discussed with young people and their families, and strategies are put in place to prevent nocturnal hypoglycaemia, such as a low-glycaemic-index evening meal, bedtime snack incorporating carbohydrate and protein (Paterson et al, 2016), and bolus and basal insulin reductions (Robertson et al, 2014; Riddell et al, 2017).

Outcomes and future plans
The feedback from the gym staff was extremely positive and they wish to put future staff through the training. They are also keen to facilitate group exercise sessions for young people with diabetes, which is something we hope to enable in the future. We also hope to roll this out to gyms in other local boroughs where leisure facilities offer gym membership for young people.



Study provides new clues to why this condition is more aggressive in young children.
14 Nov 2025