

The prevalence of diabetes is at an all-time high, with over 5.6 million people estimated to be living with the condition in the UK, around 90% of whom have type 2 diabetes (Diabetes UK, 2023). Around one in six hospital beds are occupied by people with diabetes, although most are admitted for conditions unrelated to diabetes.
Hyperosmolar hyperglycaemic state (HHS) is a rare but potentially life-threatening medical emergency that occurs more typically, but not exclusively, in older adults with type 2 diabetes (Joint British Diabetes Societies for Inpatient Care [JBDS-IP, 2022]). Following an incident of an inpatient developing HHS in one of the Care of the Older Person wards of the NHS University Hospitals of Liverpool Group, an audit was conducted to assess the diabetes knowledge of the ward staff. This article outlines the process, the findings of the audit and subsequent action to address the gaps in knowledge that were identified.
Hyperosmolar hyperglycaemic state
Although it accounts for <1% of all diabetes-related admissions, HHS has a mortality rate of up to 20%, significantly higher than that of diabetic ketoacidosis (DKA; French et al, 2019; Mustafa et al, 2022). HHS develops more slowly than DKA (over many days) and is driven by extreme levels of hyperglycaemia and consequent osmotic diuresis and hypovolaemia, but without significant ketonaemia or acidosis. Common symptoms are polyuria, polydipsia, weakness, weight loss, tachycardia, dry mucous membranes, poor skin turgor and hypotension (French et al, 2019). In severe cases, a person may present with confusion or shock (French et al, 2019). High serum osmolality is associated with altered levels of consciousness that can lead to coma, although this is rare (French et al, 2019; Adeyinka and Kondamudi, 2023).
Precipitating factors include acute infections, cardiovascular events, steroid (glucocorticoid) therapy, inadequate fluid intake and the discontinuation or omission of antidiabetes medications (French et al, 2019; Mustafa et al, 2022). Treatment goals are to address the underlying cause, gradually normalise osmolality and blood glucose, and replace fluid and electrolyte losses (Joint British Diabetes Societies for Inpatient Care [JBDS-IP], 2022).
As HHS occurs most usually in older adults with type 2 diabetes, it is uncommon for nurses on non-diabetes wards to encounter it. However, as the UK population ages and the number of people with undiagnosed type 2 diabetes increases, the likelihood will increase. There is also evidence that adherence to steroid pathways and JBDS-IP standards is patchy (Amusan et al, 2019), and that rates of preventable inpatient-onset HHS and DKA need improvement (NHS England, 2020). For an inpatient being initiated on steroids, the nursing staff need to be informed to conduct capillary blood glucose (CBG) checks, even if there is no pre-existing diabetes diagnosis. The JBDS-IP (2023) provides guidance on how to assess hyperglycaemia in people taking steroids with different clinical needs.
Methodology
The incident mentioned above relates to an 82-year-old inpatient who developed HHS in October 2024 owing to prolonged steroid treatment without adequate CBG checks and with the likelihood of underlying type 2 diabetes. Once HHS had been identified, treatment resolved it after two days. A Datix incident report highlighted the need for improvement in CBG checking for patients on steroids, in action taken when CBG is high and in staff knowledge of fixed-rate insulin infusion (FRII) and variable-rate insulin infusion (VRII). A recent Liverpool Hospitals Quality Assessment internal review of the ward had also recently shown the need for improvement in knowledge of hypoglycaemia.
Subsequently, the lead author devised a snapshot audit to determine the diabetes knowledge of the ward staff.
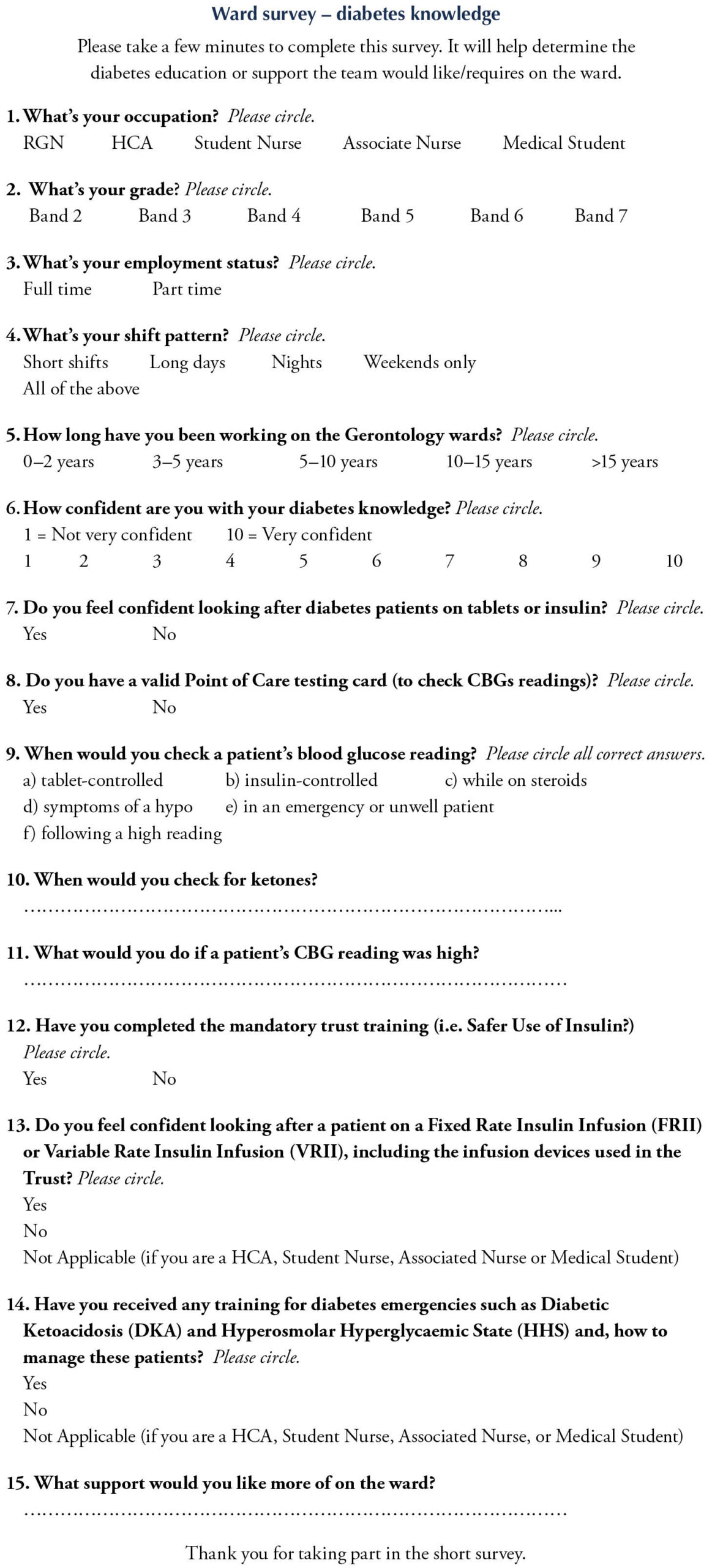
The survey asked staff about their:
- Level of nursing experience and training in diabetes care.
- Confidence in their knowledge of diabetes.
- Knowledge on checking CBG and ketone levels (Appendix A).
Consent to conduct the survey was obtained from the Consultant and Ward Manager, and it was registered with the Trust Clinical Audit Management Systems. This was a voluntary and anonymous study, so no personal details were collected and any completed survey implied informed consent. Conducted over one week, the survey was circulated to both day- and night-shift staff, and could be completed in paper or electronic format. To improve engagement, the survey was promoted on a work WhatsApp group and reminders were sent every other day. A designated area was available for paper copies to be returned.
Results
The survey was sent to 52 permanent clinical staff based on the ward. Of the 43 (83%) who completed it, the 22 (51%) were registered nurses (RGN; Bands 5–7), 15 (35%) were healthcare assistants (HCA; Bands 2–3) and 6 (14%) were student nurses. There were no associate nurses or medical students on the ward during the week of the survey. Of those surveyed, 34 (79%) were employed full-time. Long day shifts were worked by 21 staff members, mixed shifts by 16, nights by 11 and short shifts by 4.
While 53% of the RGNs and HCAs had only 0–2 years of experience on the Care of the Older Person ward, 12% had over 15 years of experience. Self-scored from 1–10, the average ward score for confidence in diabetes knowledge was 6.35, with 32 (74%) scoring themselves from 6–10. Most of those scoring themselves from 1–5 were HCAs. When caring for diabetes patients on tablets or insulin, 33 (77%) felt confident.
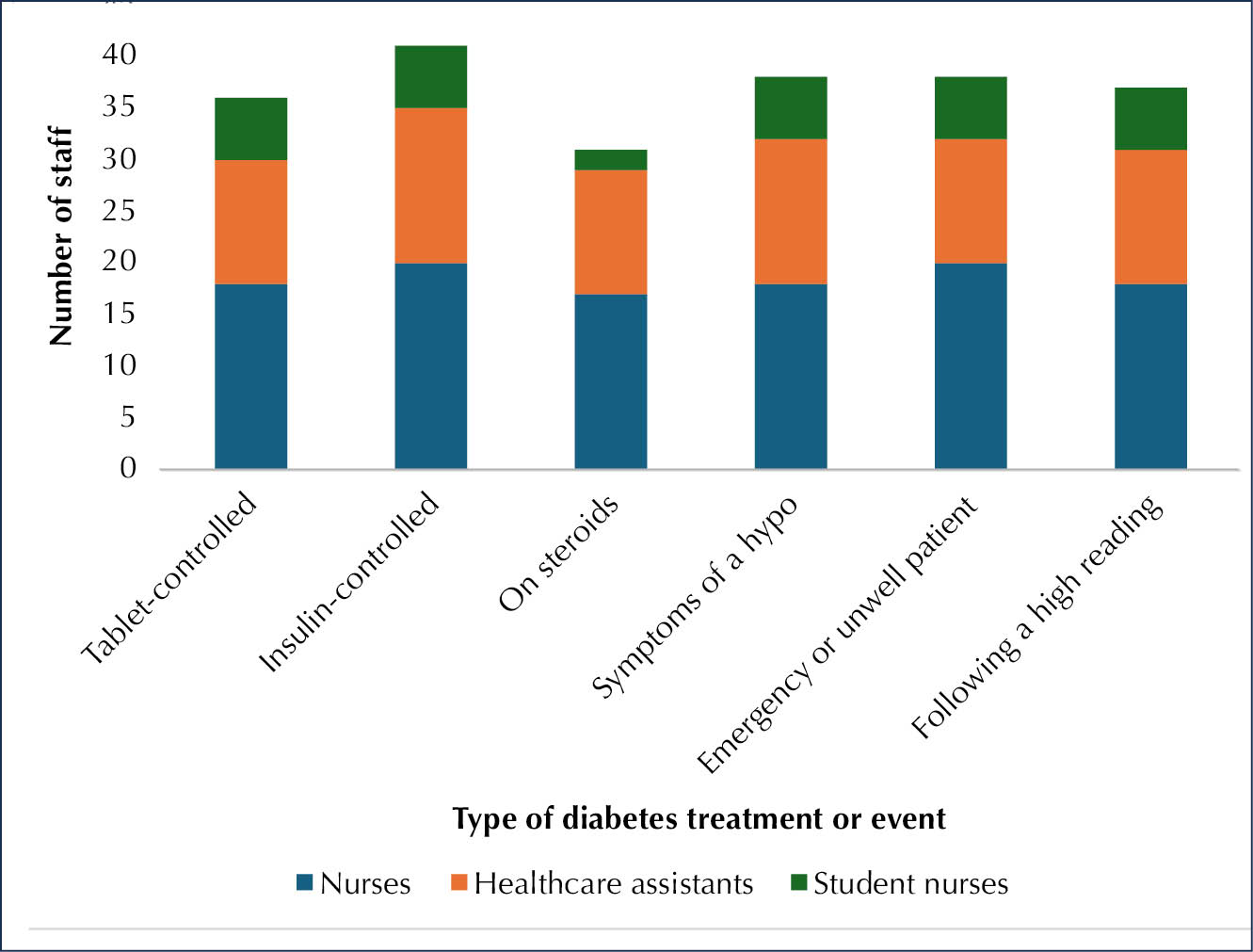
When asked to choose in which of six given situations they would check a patient’s CBG reading, 41 (95%) responded that they would for those on insulin, while 31 (72%) responded that they would for those on steroids (Figure 1). Most RGNs correctly selected all six situations, although two selected only one answer. Most of the HCAs selected 3–5 situations, although three selected only one answer. Two of the student nurses selected all six, while the other four chose five situations.
When provided with an open-ended question about when they would check for ketones, 33 (77%) said they would check when they notice a high CBG reading or if the patient was unwell, with 14 (33%) quoting specific CBG readings ranging from 14 to 20 mmol/L. Ten (2 RGNs and 8 HCAs) did not know when to check for ketones.
When staff were asked what action they would take if a patient had a high CBG reading, they said they would:
- Inform the medical team, nurse in charge, advanced clinical practitioner (ACP) and/or diabetes team (n=25).
- Check the patient’s blood or urine ketones (n=12).
- Recheck CBG (n=9).
- Check current diabetes medications (n=8).
- Check oral intake for sugary foods, snacks or drinks (n=5).
- Encourage patient to drink more water (n=2).
When considering training, 65% (21 RGNs, 4 HCAs and 3 students nurses) had received CBG testing training and had a valid Trust Point of Care Testing (POCT) card. Regarding the Trust’s mandatory safe use of insulin training, 75% (19 RGNs and 2 student nurses) were up to date. However, only 12 RGNs had received VRII or FRII training and only 7 RGNs had received DKA or HHS training. When asked what further training they would like on the ward, staff requested instruction on VRII, FRII, DKA, HHS, hypoglycaemia, insulin and managing different types of diabetes patient.
Discussion
A strength of this snapshot audit is that the majority of the ward staff (83%) completed it. Around half of the respondents reported working long days, which can mean that there is less time to complete activities that support good nursing practice (Emmanuel and Ball, 2023). Support from the managerial team is, therefore, important to ensure that staff training is up to date. As over half of the RGNs and HCAs had only 0–2 years of experience (and few had more than 15 years), there is a need to provide staff with the clinical skills to manage patients with diabetes.
The reported scores suggest that staff had a reasonable confidence level when caring for diabetes patients. A large proportion recognised that CBG should be checked for a patient taking antidiabetes tablets or insulin, if they had hypo- or hyperglycaemic symptoms, or in an emergency. However, it was concerning that a patient on steroids was the category least recognised as requiring CBG testing, given that such a patient developing HHS prompted the audit.
The majority of the staff had completed the Trust’s safe use of insulin training and had a valid POCT card, with most of them being able to recognise high CBG readings and respond safely. However, other responses highlighted the need for further training in VRII, FRII, DKA and HHS.
Although staff on this ward generally had a good understanding of diabetes care, they recognised the need for further training. This is particularly important on a Care of the Older Person ward.
All things considered, staff on this ward had a good understanding of diabetes care, although they recognised the need for further training for them to provide the best care for their patients. The British Geriatrics Society (2023) has stated that around two-thirds of hospital inpatient beds are occupied by an older person, so it is imperative for the most senior and experienced nurses on the ward to support more junior staff in improving their overall diabetes knowledge.
Follow-up
The audit findings were presented to the Ward Manager and nursing team and then to the ward’s medical team and Assistant Director of Nursing for the Department of Geriatric Medicine and Diabetes & Endocrinology in November 2024.
Following this, the Ward’s ACPs, Manager, Sisters, and Practice Educator met to create a strategy to upskill the ward staff. It was agreed that we would enhance this collaborative working further by linking in ward education sessions with the support of the inpatient DSN, Specialist Biomedical Scientists in Point of Care Testing and Acting Ward Sister for the Diabetes ward.
Consequently, educational sessions on VRII, FRII, DKA and HHS were run biweekly for one month. The following month, the POCT delivered training on the ward biweekly on both CBG and ketones. As training was delivered on the ward, these were run at 12.30–2.00 p.m., after the morning ward round and patient lunchtime, and before the afternoon medication round. Staff on night or weekend shifts were encouraged to attend when Trust group sessions where available.
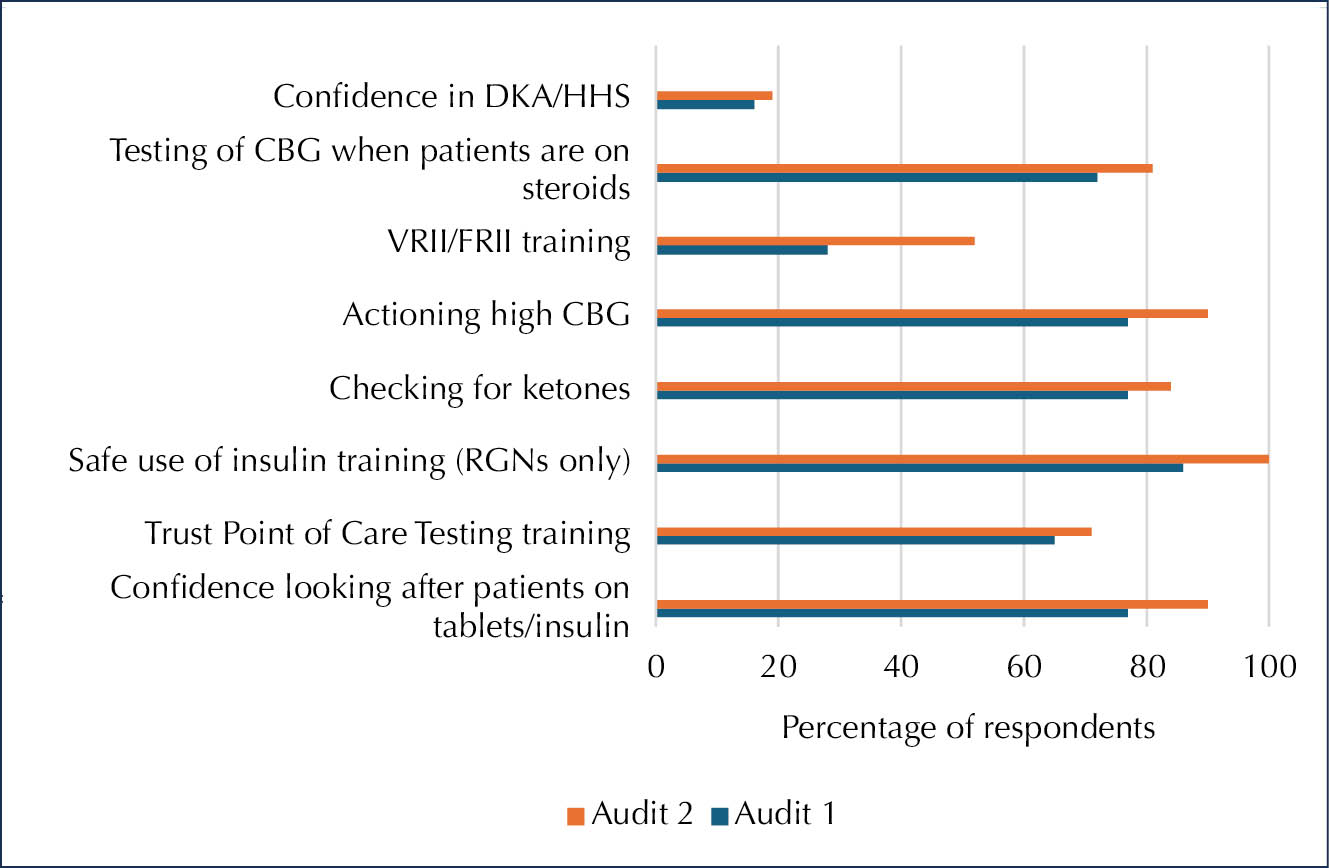
Following this collaborative working and staff education intervention, a re-audit was conducted 4 months later which showed a number of achievements:
- Confidence is diabetes knowledge increased from an average of score of 6.35/10 to 6.65/10.
- Confidence in looking after patients on antidiabetes tablets or insulin increased from 77% to 90%.
- Confidence in VRII/FRII increased from 28% to 52%, and there was a marginal improvement in DKA/HHS from 16% to 19%.
Training levels showed the following improvements:
- Uptake of POCT increased from 65% to 71%.
- The majority of the staff who knew when to check for ketones increased from 77% to 84%, and who knew the action to take for high CBG increased from 77% to 90%.
- Testing of CBG when patients are on steroids improved from 72% to 81%.
- RGN compliance with the safe use of insulin training improved from 86% to 100% (Figure 2).
Conclusions
The audit revealed that it is imperative that the most senior and experienced staff help to address gaps in knowledge of the more junior staff. The clearest need for diabetes education was shown to be on checking CBG readings for patients taking steroid medication. A need for the person prescribing steroids to a patient to inform the nurse caring for that individual to monitor CBG at least once a day and to notify them if consecutive high readings are recorded was also identified.
On a Care of the Older Person ward, all RGNs must ensure that they are up to date with safe use of insulin training. All staff should have a valid POCT card or training to monitor CBG and ketone levels. It is also suggested that the inpatient diabetes team devise and implement Trust guidelines for hyperglycaemia to aid ward staffs’ understanding of when to check for ketones and the importance of promptly requesting medical intervention.
The re-audit showed how effective collaborative working can improve diabetes knowledge, build confidence and improve patient care. All RGNs should aim to be up to date with VRII, FRII, DKA and HHS training to maintain their diabetes emergency knowledge and response. Additionally, the Ward Diabetes Link Nurses should attend all relevant diabetes Trust study days to aid the dissemination of knowledge and training on the wards.
Acknowledgements
The authors would like to thank: Chloe Lee (Ward Clerk) – for helping to collate accurate ward staff data; Elysia Gee (Ward Healthcare Assistant) – for helping to disseminate and collect ward survey responses, especially during the night and weekend shifts; Michelle Walsh and Susan Gandy (Specialist Biomedical Scientists, Point of Care Testing) – for delivering CBG and ketone training on the ward.
Appendix A



Better diabetes care central to reducing premature mortality.
15 Jul 2026