

The evolving role of pharmacists in managing long-term conditions
Over the past decade, the role of pharmacists has evolved significantly due to initiatives such as the General Practice Forward View in 2016, which committed to employing 1,500 clinical pharmacists for primary care over five years; and the Additional Roles Reimbursement Scheme in 2019, which aimed to recruit six clinical pharmacists for each primary care network (NHS England, 2016; Anderson and Francetic, 2025).
Clinical pharmacists have a range of responsibilities, including conducting structured medication reviews, medicines optimisation duties and independent prescribing. For a patient with one or more long-term conditions, the pharmacist is frequently the healthcare professional they see most often; this places the pharmacist in a uniquely privileged role in the management of these patients.
The cardio–renal–metabolic paradigm
Cardio–renal–metabolic (CRM) conditions refer to a range of interconnected conditions affecting the heart, kidneys and metabolic system (Braunwald, 2019). Type 2 diabetes (T2D), cardiovascular disease (CVD) and chronic kidney disease (CKD) commonly occur concurrently; 1.4 million CVD deaths worldwide are attributable to CKD (Carney, 2020). In the UK, 16% of people with heart failure (HF) have comorbid T2D and CKD (Vijay et al, 2022). International guidelines recognise the interplay between these conditions and recommend a multifactorial approach to their identification and management (Davies et al, 2022; KDIGO, 2024).
CKD: A growing public health emergency
Chronic kidney disease is defined as abnormalities in kidney function or structure, or both (i.e. estimated glomerular filtration rate [eGFR] less than 60 mL/min/1.73 m2 and/or urine albumin-to-creatinine ratio [uACR] greater than 3 mg/mmol) present for more than three months with associated health implications (KDIGO, 2024). Worldwide, CKD affects more than 10% of the general population and is expected to be the fifth leading cause of life-years lost by 2040 (Kovesdy, 2022). The number of people requiring dialysis in the UK is expected to rise over four-fold from 2023 to 2033 (Kidney Research UK, 2023). In high-income countries, one in three people living with diabetes, and one in five people with hypertension, have CKD (Francis et al, 2024).
Early identification of CKD
Identifying CKD early in its course is essential for reducing the risk of CKD progression, cardiovascular events and hospitalisations (Gohda and Murakoshi, 2022; KDIGO, 2024). Given the interconnected nature of CRM conditions, people with T2D and/or CVD would benefit from proactive testing for CKD. Pharmacists have an opportunity during structured reviews to identify people at highest risk of CKD; for example, annual review of a person with T2D should include assessment of kidney function and damage, alongside assessing for additional risk factors such as hypertension (NICE, 2023).
Two tests are important for identifying kidney damage early, namely eGFR, which measures kidney function; and uACR, which looks for evidence of kidney damage (KDIGO, 2024). Since kidney damage may be evident before kidney function declines (Tonneijck et al, 2017), uACR testing can provide early warning of kidney damage.
Albuminuria and uACR: An underutilised biomarker in primary care
However, since its removal from the Quality and Outcomes Framework (QOF) in 2015, uACR testing has halved in the UK (Stewart et al, 2024). According to CVDPREVENT data to December 2024, the national average of patients in England with CKD (G3a–G5) who have had uACR or protein-to-creatinine ratio testing within the previous 12 months is 49.6% (Office for Health Improvement and Disparities and the NHS Benchmarking Network, 2024). This potentially puts people with CKD at increased risk of disease progression and poor outcomes (Kanumilli et al, 2023).
Supporting people living with CKD
Alongside testing, it is important that people with CKD are coded correctly in order to support their access to appropriate care. According to the REVEAL-CKD study, 56% of patients in England whose eGFR indicated G3 CKD did not have a recorded diagnosis (Kanumilli et al, 2023). This is important since people with uncoded stage 3–5 CKD have up to a five-fold increase in mortality risk compared to those who have been appropriately coded (Stewart et al, 2024).
Care for CKD must be holistic, including consideration of all conditions, risk factors and comorbidities (KDIGO, 2024; NICE, 2021). As key members of the primary care multidisciplinary team, pharmacists are in a position where they can make individualised prescribing decisions and support a person-centred approach to the management of people with CKD.
Regular review and follow-up is necessary to track CKD progression and assess whether any changes are needed to the person’s care. CRM clinics are one potential option for patients with CKD as well as T2D or CVD. These reduce the time-burden on patients by avoiding the need to attend multiple reviews for each condition, optimise the pharmacist’s time in seeing these patients, and also support a holistic view of the person’s care.
Pharmacists as CRM champions
As well as directly supporting patients, clinical pharmacists are able to act as advocates for best-practice CKD care among their local healthcare professional colleagues, for example by using their expertise to raise awareness of the importance and ease of uACR testing. This could also include building confidence in primary care colleagues to manage people with CKD within primary care, and only referring those who would most benefit from specialist assessment. Pharmacists could also empower colleagues to discuss CKD and kidney health in their patients with CVD or T2D.
Pharmacists could also play a role in implementing practical strategies including ensuring availability of uACR testing bottles in locations where annual patient reviews take place, and developing resources such as checklists to ensure uACR and eGFR testing are included in structured reviews of people with T2D and CVD.
Conclusion: The role of pharmacists in the delivery of treatment for CKD
Pharmacists have become central to ensuring the provision of effective treatment for CKD (Figure 1), due to the emergence of effective pharmacological therapies and an increased emphasis on patient self-management and education (Ardavani et al, 2025). Pharmacists can support other healthcare professionals in the appropriate use of SGLT2 inhibitors and provide education to people with CKD about their benefits, risks, and appropriate use.
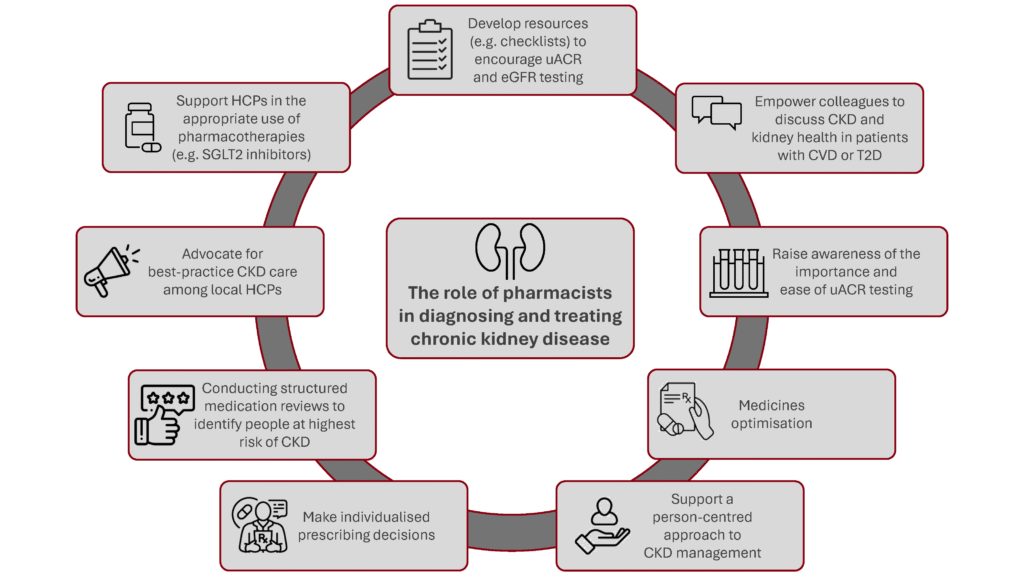
Figure created by Boehringer Ingelheim.
Want to find out more? Access further resources
 | Explore this resource hub, full of tools to support you and your patients, including videos, podcasts and downloadable resources Click to access |
 | Explore the prevalence of CKD in your local area and what support exists using this CKD Interactive map Click to access |
PC-GB-112014 | November 2025