
As children spend more than 30 hours per week in school (International Society for Pediatric and Adolescent Diabetes, (ISPAD], 2018), it is imperative that children with diabetes have optimal glycaemic control during these hours. One contributing factor to this is the education of school staff in the management of diabetes, as recommended by both NICE (2020) and ISPAD (2018). Due to COVID-19 restrictions in 2020, our normal method of face-to-face education was not possible. In response, the paediatric diabetes service at Barnsley Hospital developed a virtual school education package. This article describes how this new education package was implemented and the consequences on time, costs and user satisfaction.
Background
School diabetes education is a key part of our role as diabetes healthcare professionals. ISPAD (2018) guidelines recommended that:
“Optimal management of diabetes at school is a prerequisite for optimal school performance, including learning and for the avoidance of diabetes-related complications.”
The National Children and Young People’s Diabetes Network (NCYPDN) published a delivery plan for 2020–25, with the aim that every child with diabetes receives parity of care. Within this plan (NCYPDN, 2020), they outline the importance of establishing links with schools and providing adequate education to staff. Furthermore, the importance of school diabetes education is also included in the Royal College of Paediatric and Child Health (RCPCH) Diabetes Quality programme (RCPCH, 2019). Safety of children with diabetes is imperative, and the Department of Education (DE; 2015) has produced statutory guidance advocating that pupils in school with medical conditions should be properly supported.
Across the country there is variation in the level of school diabetes education delivered by local diabetes services. The RCPCH Diabetes Quality Programme (2019) outlines the need for a visit to school for education of staff assisting newly diagnosed children. There is, however, no set guidance as to how much education should be delivered for children with existing diabetes, or how this should be undertaken. There is a paucity of research considering the efficacy of school diabetes education.
The Barnsley paediatric diabetes service (including specialist nurses and dietitians) would normally deliver all school education face to face for all primary-school-aged children with diabetes (0–11 years). This would include one education session on diabetes management, along with three further visits to sign school staff members off as competent in diabetes management and insulin delivery. This education is not normally delivered for secondary school children as we would expect these children to be self-managing their diabetes, following the expectations in the Goals of Diabetes Education (Novo Nordisk, 2016). Education would be provided to a secondary-school-aged child, however, if the child was not self-managing or was newly diagnosed.
In 2019, this education package was completed for the school staff of 29 primary-school-aged children with diabetes, at 26 primary schools. This education was delivered between the months of June and November and equated to 7418 minutes of nurse and dietitian time.
In 2020, the team had to react to the COVID-19 pandemic and change the method of delivering this education to a virtual education package. As a team we are not yet registered with the Diabetes Quality Improvement (QI) collaborative (RCPCH, 2019). We have, however, used Lean thinking principles (NHS Institute for Innovation and Improvement, 2017) and local models of QI (Barnsley NHS Foundation Trust, 2020) to change our delivery of school diabetes education, while completing this as a local Trust QI project (Barnsley Children and Young People’s Diabetes Service, 2020).
Aims
The primary aim of this project was to develop a virtual school diabetes education package to educate 100% of school staff for all primary-school-aged children with diabetes, without compromising safety, knowledge-sharing, engagement or efficacy.
The secondary aim of this project was to evaluate how providing virtual rather than face-to-face education impacts costs, time and travel.
Method
Initially in May 2020, the team mapped out the current process and the required changes to school diabetes education using the local Trust improvement pathway (Figure 1; full version available in Appendix 1).

We initially searched to see if any virtual education materials were available to use in the modification of the education programme, however, the team was unable to find resources that met all the aspects of care and in the right literacy level for the local populations needs. In Barnsley, the level of literacy is lower than the national average (Barnsley Metropolitan District Council [MDC], 2016). As such, a decision was made to develop and produce a series of videos to replace the face-to-face education.
In total, there were 13 education videos produced between May and August 2020, and they were uploaded on to a video-sharing platform to enable easy accessibility (Barnsley Paediatric Diabetes Service, 2020). The videos produced included step-by-step carbohydrate counting, using different glucose meters and insulin pumps, and insulin injection techniques. The videos were specifically made for the Barnsley population, considering the lower-than-average literacy skills (Barnsley MDC, 2016) and high English-speaking population (98.1% English-speaking from 2011 census).
The team obtained a key contact and email address from 28 primary schools where there was at least one child with diabetes. In September 2020, an email was sent out to all school contacts with the personalised diabetes school care plan and links to the appropriate videos to enable staff to engage with this programme. This was followed up by three video-call sessions (for each school contact) from the diabetes nurses to ensure understanding of the video content and to do a virtual sign-off for diabetes management and insulin competency. For all 31 primary-school-aged children, this virtual package was delivered between September and November, 2020. It was agreed that for any child with newly diagnosed diabetes, the initial part of the school education would remain face to face, so staff could practise with both the insulin administration and blood glucose monitoring equipment.
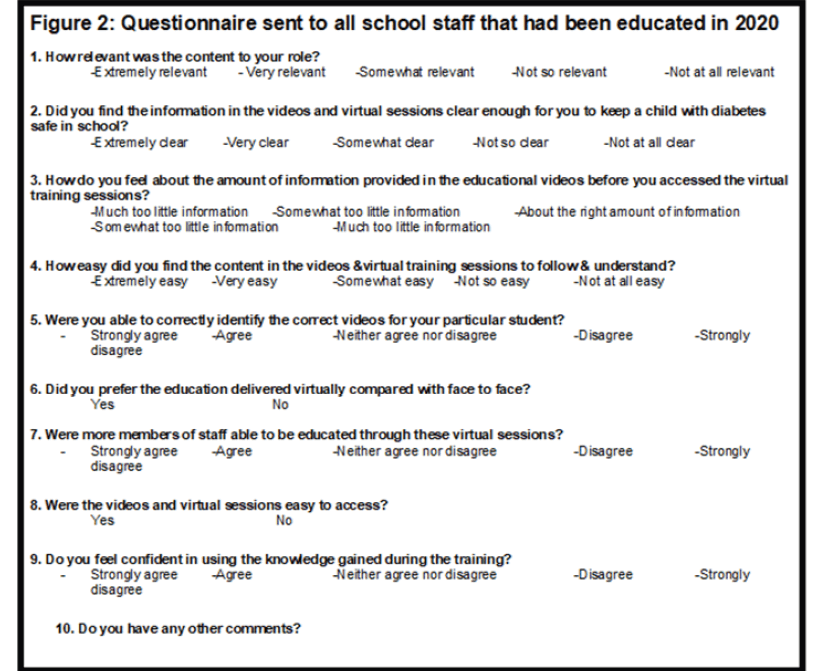
In October 2020, in order to evaluate this process, a SurveyMonkey questionnaire (Figure 2) was developed and distributed by email to all 35 school staff members who received the training. To further evaluate the process, the time and costs were audited by extracting data from the Trust’s contact recording software and amalgamated into an Microsoft Excel spreadsheet.
Findings
All of the primary schools (n=28), with a total of 31 children with diabetes, engaged with the virtual school diabetes education between September and November 2020. The numbers were comparable to those educated in 2019, where there were 29 children in 26 schools.
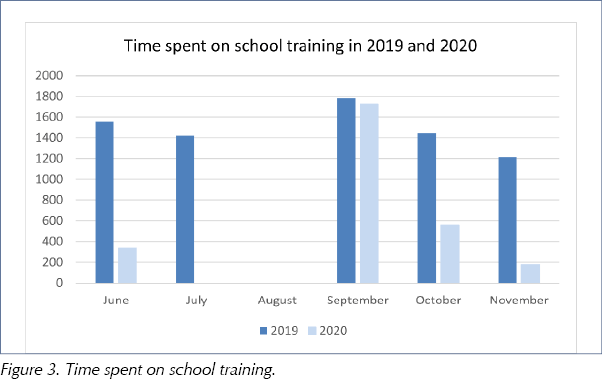
Comparison of the time spent on school education showed that the team spent a total of 7418 minutes in 2019 (equating to 124 hours or 16.5 working days) travelling to, and delivering, the face-to-face diabetes education. In 2020, the time spent on school education was 2802 minutes (47 hours, or 6.5 working days), equating to a time saving of 62.2%, or 10 working days. The reduction in work time for Band 6 or 7 nurses led to a cost reduction of approximately £1420 per year.
The education in 2020 was undertaken mainly in September, whereas in 2019 this was more evenly distributed amongst the months from June to November (Figure 3). This meant that in 2020 the other months could be spent on other aspects of diabetes care and service improvement.
The mileage that had been undertaken in both years was also reviewed. In 2019, the team drove a total of 1248 miles (£715.90), whereas in 2020 they drove 186 miles (£103.95). This equates to a reduction of 85% in mileage in 2020. Although the team had planned to deliver all sessions virtually, there were a small number of school diabetes education sessions that needed to be face to face, due to newly diagnosed children. Over time, a reduction in driving and mileage would have a positive impact on our carbon footprint and the environment (Ivanova et al, 2017), as well as significant cost savings.
Questionnaire findings
The team received 17 responses (48% response rate) from the questionnaire sent to school staff. This response rate was higher than our team anticipated, as school staff were under additional pressures at this time with the COVID-19 pandemic, meaning some staff were self-isolating. Although a 48% response rate lacks statistical power, the replies do give a clear idea of how staff found this new education delivery method. The findings were positive overall and there were no concerning comments. When asked how relevant the education package was to their role, 100% of respondents responded “extremely or very relevant”.
All respondents said that they found the information either “extremely clear or very clear”, in response to keeping a child with diabetes safe in school in accordance with the DE (2015) guidelines (Figure 4).

Figure 5 shows that 88% of respondents found the content of the diabetes education either “extremely easy or very easy to follow and understand”, and all participants were able to identify which videos were needed for their students.

Figure 6 shows that the majority of respondents (82%) felt confident in using the knowledge gained; however, one respondent (6%) disagreed with this and reported that they did not feel confident. All staff were provided with three video-call sessions to enable them to ask questions and check understanding.
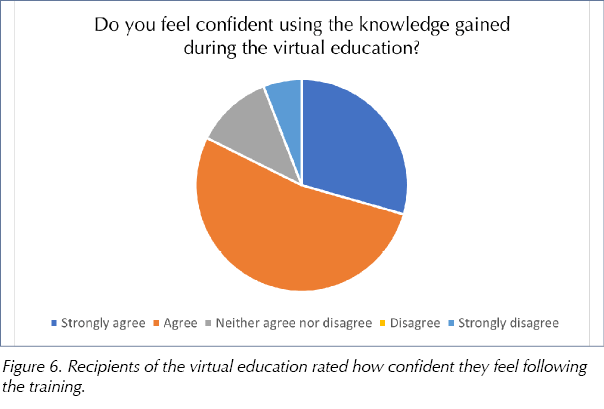
As the questionnaire was confidential, we were unable to identify the respondent who did not feel confident and, as such, were not able to follow up.
When asked whether the virtual sessions allowed more staff members to receive education, 65% of respondents agreed, but 12% disagreed. When asked if they preferred the virtual delivery compared to face to face, 63% preferred the face-to-face delivery. As a team, we considered if this was because schools were used to the education being delivered in person and change can be difficult. We also considered the large amount of changes happening in schools in 2020 due to the pandemic.
Discussion
When we directly compare the two delivery methods, there are significant savings in both costs and time. The total cost savings in 2020 was £1420 in time and £611.95 in mileage, totalling £2031.95. The time savings were equivalent to 10 working days. We found that the actual time spent with school staff was equivalent, as face-to-face sessions and virtual sessions are comparative in duration. The largest benefit to delivering the virtual education was the reduction in travel time and mileage costs due to our large geographical area. Considering Lean Principles (NHS, 2017), travelling to schools would be seen as a non-value-added step if virtual school education can be undertaken with the same results.
Considerations for future practice
Overall, the feedback received showed that school staff felt it was easier to access virtual education, as there was no set time and content could be repeated. Initially, it was found that there were perceived problems with accessing virtual education, but this improved as staff got used to this method. In the audit post-education provision, 63% of respondents commented that they preferred face-to-face education. Despite this figure, this would not be a strong enough reason to change back to face-to-face education in the future. The team would ensure, however, that it continues the video-call follow-on sessions, so that school staff have a chance to ask questions and interact. Furthermore, we can continue to check their competence and understanding.
Overall, the diabetes team did not feel that diabetes education could ever be completely replaced with a virtual system, as it is important to provide an interactive platform. The significant cost savings, time savings and overall feedback strongly suggest, however, that it is beneficial to provide the majority of this training virtually.
The videos created have also been used in ward-training sessions, and with educating newly diagnosed children and their carers. This further substantiates the benefits of creating virtual resources for children with diabetes.
Conclusion
The team has discussed the time and cost efficiencies and has decided that the majority of future school diabetes education will be delivered virtually. This method then allows us to use the time saved to deliver other aspects of paediatric diabetes care and service development.
This local QI project could be extrapolated as a regional research project across different diabetes teams and different populations throughout this next year, to develop and share innovative practice across the diabetes network.
Acknowledgements
The following people are members of the Children and Young People’s diabetes service at Barnsley Hospital NHS Foundation Trust:
- Sam Norris, Paediatric Diabetes Nurse Specialist.
- Joanne Cave, Paediatric Diabetes Nurse Specialist.
- Emily Ellis, Paediatric Diabetes Nurse Specialist.
- Kirsty Roberts, Paedriatric Diabetes Dietitian.
- Dr Bhimsaria, Paediatric Diabetes Consultant Clinical Lead.
- Kate Pattison, Paediatric Diabetes Admin Support.
With thanks
The author thanks the Quality Improvement Team, Barnsley Hospital NHS Foundation Trust; Communications Team, Barnsley Hospital NHS Foundation Trust; and Birmingham City University, as part of the LBR7587 Collaborative Children and Young People’s Diabetes Care Module.




NHSEI National Clinical Lead for Diabetes in Children and Young People, Fulya Mehta, outlines the areas of focus for improving paediatric diabetes care.
16 Nov 2022