
Emerging adulthood is a particularly vulnerable period during which individuals go through great change, which can be further complicated by the daily demands of diabetes. It is clear that there is an increased risk of adverse outcomes at this stage in life, which is in part due to decreased adherence to self-management (Dunger, 2017).
In England, the Best Practice Tariff (BPT), a tariff from the Year of Care programme, introduced certain criteria and care processes to incentivise the delivery of high-quality paediatric care to all children with diabetes. This may work well to improve care up to the age of 19 years; however, while a high proportion of people with diabetes complete their care processes as children and teenagers, this rate falls quite markedly at 20–24 years of age (NHS Digital, 2019).
In 2012, Poole Hospital’s adult and paediatric diabetes teams recognised the needs of young people and, using the BPT funding available for patients aged 15–19 years, wrote a business plan for a specific diabetes transition service to help bridge the gap between paediatric and adult services. The Young People’s Diabetes Service (YPDS) team sits within the adult diabetes service at Poole, rather than the paediatric service, to make sure the movement into adult services is as smooth as it can be. The existing, limited service was redesigned into a transition-specific service to work effectively for young people, being flexible to their needs and lifestyle:
- The young people must get a chance to get to know the team looking after them.
- The healthcare professionals involved in the service must listen to young people and be able to offer them tailored advice.
The service was further redesigned in 2014/2015, with key stakeholders including the children’s diabetes service, the adult diabetes team, and young people and their families/carers. The initial and ongoing aim was to improve the care of diabetes for young people, and to measure this improvement through achievement of the BPT, reductions in HbA1c and increased attendance at clinics. Another key aim of the service with regard to safety was to identify young people who had been “lost to follow-up” and to keep them under review even if they chose to disengage.
In the first few months, team members interrogated the different hospital computer systems to build a potential caseload of 15–25-year-olds. However, the maximum age was later reduced to 23 years as the total number of young people in this group was higher than expected, with a large number of young people due to join the service from the local paediatric team, and capacity had to be considered. Those young people who had disengaged were invited back into the hospital-based clinic.
The team structure evolved between 2014 and 2018, and the team is now made up of:
- Two consultant diabetologists (contributing 1.25 sessions per week between them).
- One consultant paediatrician with a specialist interest in diabetes (one session per month).
- One Band 7 diabetes transition nurse specialist (1 whole time equivalent [WTE]).
- One Band 3 information assistant (0.5 WTE).
- One Band 8a diabetes clinical psychologist (0.2 WTE).
- One Band 6 diabetes specialist dietitian (0.4 WTE).
A consultant diabetologist is responsible for leadership of the team, but each and every member is responsible for the care provided to the young people, with the key to the team’s success being a flat hierarchy in which every team member contributes ideas, innovations and developments.
Patient-centred care
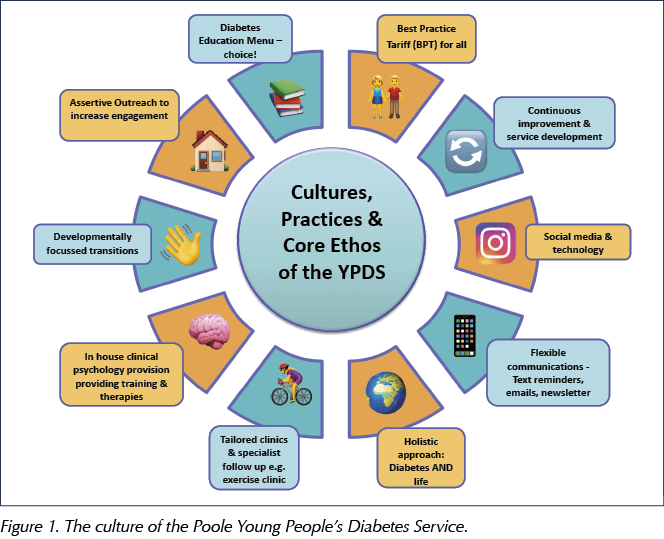
The YPDS team has imbedded a culture of continuous improvement (see Figure 1) and, as the service has evolved, the following changes have been introduced.
Clinic support
- Weekly afternoon clinics for young people introduced, with additional urgent slots to facilitate a review when needed.
- Monthly evening clinics to offer flexibility for college- and work-aged young people, with annual review appointments offering a “one-stop shop” for consultant, dietetic, psychological and DSN review.
- Creation of a weekly, nurse-led clinic for those aged 19 years and over, which specifically supports with the transition to adult services.
- Weekly dietetic clinic.
- All clinics are holistically driven, with the team focusing on developing relationships with the attendees and finding out about more than just their diabetes.
- Development of a database to closely monitor HbA1c and clinical outcomes, and to flag any areas of concern.
- Day-to-day management of the clinics was transferred to the YPDS, rather than sitting with the hospital outpatients department, allowing slots to be reallocated at short notice according to the clinical need of the young people.
- Poole Diabetes Centre is used by the paediatric team one afternoon a week so that, as young people move into the transition service, they already know the layout of the clinic and many of the people who work in and with the YPDS team.
- Incorporation of psychological skills into consultations:
– Weekly clinical psychologist clinic, offering evidence-based psychological therapies.
– Regular case discussion meetings for the multidisciplinary team to psychologically formulate what might be going on for young people and how best to approach support, including ongoing safeguarding issues and assessment of risk-taking behaviours.
– Psychological skills training for staff.
– Part of multidisciplinary team at weekly and monthly consultant clinics.
Outreach
- Active case-finding for young people not attending or disengaged from the service.
- Home, work, school or college visits if required.
- Liaison with departments outside the hospital – social care, housing, police, prisons, community mental health services, sexual health services, benefits agency and local drug and alcohol support teams.
Communication
- Text and/or email reminders for all YPDS clinic appointments. New attendees are asked to fill in a contact form (Figure 2), and to check their details every time they are seen so the service has the best chance of keeping up to date.
- Text, email and telephone helpline provided for young people, including out-of-hours advice for those below the age of 19 years.
- Quarterly newsletter sent via email.
- Poole Hospital-based website which is regularly updated.
- Trust-supported Instagram account from November 2018, offering service updates and signposting to diabetes education and the latest diabetes news updates.

Education
- “Education menu” developed to give young people a choice of how they want to receive diabetes education (group sessions, college clinics, online or one-to-one education, or none at all).
- Quarterly bite-sized education and topic-specific information, including websites, blogs, apps and social networking tips, are emailed out to those who choose the “online learning” option on their education menu.
- Monthly Poole College clinics – development of a group education programme with a curriculum and lesson plans aligned to the With You All The Way type 1 diabetes education package for 16–18-year-olds (Novo Nordisk, 2016). All of the Living with Diabetes topics are covered over a 2-year period and a small number are repeated annually as they are so popular (e.g. alcohol, travelling, driving and festivals).
- Liaison with universities and offering Disabled Student Allowance letters of support.
- Dietetics questionnaire in which young people can choose topics that need more discussion with a dietitian.
Transition
- Transition is developmentally set, with conversations about readiness to move on to adult services happening at different times for different young people, depending on when they feel ready.
- Consultant paediatrician embedded into the YPDS team.
- The YPDS nurse and dietitian work with both the paediatric and adult services, so they have met and know the young people before they transition into the YPDS.
- The team developed a biopsychosocial assessment tool which is completed by young people who have newly transitioned from the paediatric service or those coming to the service from elsewhere, so that, with discussion, we are able to find out about the young person, and not just about their diabetes. The tool assesses areas including the individual’s family structure, educational background and current level of self-management.
- Quarterly handover meeting with the Adult Diabetes Service, and a link adult DSN allocated to each young person based on their GP practice.
- Quarterly meetings with the Trust safeguarding leads for supervision and any updates needed.
- Step-up form developed and completed with the young people if they move away from the area (Figure 3).

The YPDS has a driven, “can-do” attitude, allowing rapid cycles of change and evaluation to assess what works and what does not, with involvement from the young people in these decisions. A good example would be the education menu developed by the team, which asked individuals to select how they would like to receive education. Contrary to the views of many healthcare professionals, and national guidelines, very few young people selected group education, and this allowed the team to plan the delivery of education to this cohort, according to their needs and wishes, which may be different to education planned in other age groups.
Patient-centred care using 21st century technology (e.g. online education, insulin pumps, continuous and flash glucose monitoring) is a key component of the team’s success and ensures that the team develops initiatives that are designed with young people in mind first, not solely what is the most convenient for the healthcare team.
The quarterly business meeting enables areas of clinical governance to be discussed to ensure the service remains safe and effective. During this meeting, complaints and any clinical incidents that have occurred are considered. Planned audits using Plan, Do, Study, Act (PDSA) cycles are designed to benchmark and improve care.
Clinical outcomes
The success of the YPDS has seen improvement in diabetes control in young people aged 15–23 years, with the mean HbA1c reducing from 80 mmol/mol (9.5%) in 2013/2014 to 73.3 mmol/mol (8.9%) in 2017/2018. Rates of non-attendance at clinic appointments have dropped from 19.8% to 15.5% between 2015/2016 and 2017/2018, and diabetes-related hospital admissions have also dropped from 34.7% to 16.9% between 2014/2015 and 2017/2018.
We have seen that building flexibility with frequent contact, imbedding the philosophy of assertive outreach and striving to design a service that is focused on young people can achieve great improvement for those living with diabetes. However, there is a recognition that all services need to reassess and work to improve wherever possible.
Continued improvements and future plans
The service strives to continually involve children, young people and their families/carers in the service design. This can be challenging but below we have detailed our efforts to remain focused on the young people and involve them in all we do:
- Education menu:
– Audit of the menu has shown that, although young people tend to choose online education, they do not go on to complete it. This has challenged us to make sure that the digital options we provide are up to date, and to respond to the gap between wanting to pursue digital education and the barriers to completing it. As a result, we now send out “top tips” emails covering different education topics, and are developing the use of social media to further bridge that gap. - Utilising lesson plans and resources from the college clinics in monthly hospital clinics:
– Safe alcohol advice in Nov/Dec; glycaemic index in Jan/Feb; exams advice in Mar/Apr; travel and festivals in May/Jun; going to university, leaving home and contraception options in Jul/Aug; and driving with diabetes in Sep/Oct. - Dietetics questionnaire:
– Although many of our young people choose to discuss diet at the clinic, fewer want to see a dietitian to discuss this. We are trying to develop ways to make the information accessible to all in formats beyond a clinic setting, and this includes the bite-sized, topic-specific information and top tips. - Social media/virtual clinic questionnaire:
– We invited young people to complete an online survey and had conflicting results about whether they would like a Young People’s Diabetes Facebook page, so we have not developed this. The respondents did say that they would engage with the Instagram app, so we have recently set up one of the first department Instagram pages in the Trust: @poole.ypds
– The young people have been clear that they do not want Skype consultations, so we have not developed this. - Sharing best practice:
– Team members have been asked to deliver talks at network meetings and national conferences on our transition model and results.
– Recognition from the Quality in Care Awards 2018 and most recently the BMJ Diabetes Team of the Year Award 2019.
After identifying significant variation in the quality of the service provided across the county, the Poole YPDS team are currently working with Dorset Clinical Commissioning Group (CCG) to share the work we do. The ambition for this work is that it will be scaled up throughout the county in line with the CCG’s plan to develop a single diabetes service across the region. We are also currently involved in Diabetes UK’s Wessex Diabetes Transition Change Lab and are holding our own Dorset-wide transition stakeholder events, with a view to develop a Dorset-wide diabetes transition service in the coming years.
Summary
Paediatric BPT funding was used to expand the Poole YPDS serving patients aged 15–23 years, creating a developmentally appropriate service for this group. Developing trusting and supportive relationships with young people is at the heart of what we do in the delivery of holistic diabetes care. Since 2014, Poole YPDS has achieved improved HbA1c and greater engagement with the service, with fewer missed clinic appointments and fewer diabetes-related hospital admissions.
Our YPDS team is happy to share resources with other teams if requested and can be contacted on YPS.diabetes@poole.nhs.uk




{kind=link}
Helping homeless adults to overcome the challenges of managing their condition.
16 Apr 2024