
In 2015 it was noted that there was an increase in Datix incidents related to diabetes, including four serious incidents that required investigation and root cause analysis. Four common themes emerged from these investigations: lack of knowledge and awareness of diabetes; lack of blood glucose monitoring and/or appropriate action; lack of awareness and/or adherence to guidelines; and lack of escalation.
A working group, chaired by the Chief Nurse, was set up to improve the education and training of frontline staff. Among the various main changes and initiatives was the establishment of a unique Diabetes Nurse Educator role in 2015.
The aim of this article is to share my experiences as a diabetes educator in a large NHS hospital. I will outline my personal journey of developing my own diabetes knowledge and, eventually, developing the confidence to teach others about diabetes. My role has now evolved and I continue to play a central role in education, including mentoring my successor.
How it all came about
I have been a registered adult nurse since 2002 and have always enjoyed education. Consequently, I have worked as a practitioner–health lecturer, a clinical practice educator and a clinical educator before coming into this role. I responded to the job advertisement for a diabetes educator in 2015 because I was looking for a different challenge. However, reading the advert, I was acutely aware that I did not really know much about diabetes. As a ward nurse, I have administered insulin and checked blood glucose levels, and as a clinical educator I supervised and assessed newly qualified nurses as they administered insulin to patients; however, I did not have much insight into diabetes itself. I was nonetheless hopeful when my soon-to-be manager assured me that she was looking for someone with education expertise, and that the successful candidate would learn about diabetes on the job.
I was delighted when I was appointed, but this was juxtaposed with the awareness that I had a steep learning curve ahead of me. I suddenly experienced a reversal of Patricia Benner’s (1984) “novice to expert” pathway; I had cultivated experience and scholarship in education but now I had joined a speciality of which I had very little knowledge – I became a novice again. However, I had a number of experienced mentors who, along with a supportive line manager and the whole diabetes team, facilitated my diabetes learning to a point where I felt credible when teaching nurses.
My learning consisted of shadowing colleagues in clinics and on the wards, attending diabetes conferences and study days, and completing a diabetes course at a local university. I also dedicated a lot of my own time to learning about diabetes. This role coincided with my Master’s degree in education studies, in which I learned that leading in educational strategy involves both working with the status quo and also being innovative and risk-taking. In the case of diabetes, my educational plan was to embed ward-based diabetes learning to supplement classroom education.
One of my initial priorities was establishing good working relationships with staff and ward managers in my new role. I had the benefit of a good rapport with many of them from my previous role within the same hospital. I therefore spent a lot of my early months visiting wards and establishing a presence. I took the opportunity to find out from staff, informally, how they felt about diabetes and what aspects they struggled with. I dedicated the majority of my ward time to the diabetes ward, sitting in at handover and working alongside nurses and observing their diabetes care. Initially they were cautious around me, but I made it clear to them that I was there to support them in their diabetes care, and we established a rapport and they began to ask me questions. I feel that being present and available to ward staff is a key component of the diabetes educator role. Later, I also spent time on other wards, particularly when there had been a diabetes-related error or incident. My attitude has always been to be firm but approachable, rather than hostile, and I find that staff respond better to such an approach.
Educational initiatives
Some of my routine responsibilities as a diabetes educator involved administrative duties, such as booking rooms for classroom sessions and devising teaching rotas for the diabetes team. I initially thought that, as the educator, I was obliged to do all the teaching, but my line manager assured me I would have the support of the whole diabetes team. I thought it was really important for members of the team to share their wealth of knowledge and experience in diabetes. As part of my learning, I sat in on most of the sessions, having set up the rooms beforehand. Because I had made changes and introduced activities in the classroom sessions, attending them helped me to evaluate whether or not my interventions were working. Linked to this was maintaining records of attendance at diabetes sessions and creating reports when evidence was required to show how much staff engagement there had been with diabetes.
After establishing a presence on the wards, my other goal was to standardise the key diabetes messages that the team was presenting to nurses. When I had attended the one-day diabetes course as a learner, I noticed that each of the diabetes nurses would spend time logging onto the computer and opening their own version of a presentation. Learner evaluations reflected my thoughts that there needed to be a central bank of presentations with collectively agreed content. This was done, and the “new-look” one-day course became the core diabetes study day. The content was revamped to cover salient diabetes topics as well as those that reflect the previously mentioned serious incidents. A new component was to introduce more participatory methodology in the classroom sessions in order to maintain interest and promote learner engagement. For example, I had observed the use of electronic voting pads in mandatory training sessions, so I sought and was granted funding for the purchase of Turning Point® voting pads. The voting pads are used as an interactive tool to assess learning during the course of the session, and assessment data can be used as a surrogate marker to evaluate the impact of educational interventions.
Educational resources
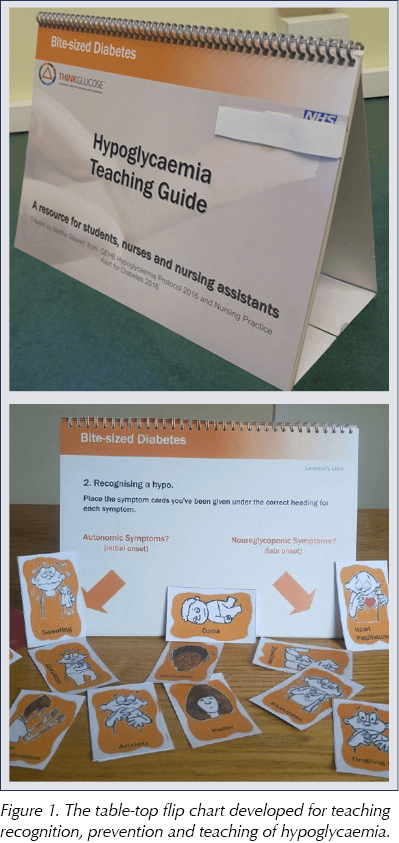
Creating educational resources was one of the most enjoyable aspects of the diabetes educator role. I personally enjoy being creative, ensuring that learners grasp any abstract concepts and can apply the information in their practice. One of the early resources I devised was a table-top flip chart for teaching recognition, prevention and teaching of hypoglycaemia (Figure 1). This came about from encountering a number of mismanaged hypos on wards and, therefore, a need to introduce short, ward-based, “bite-sized” sessions. I have discussed the flipchart in detail in this Journal (Stewart, 2017).
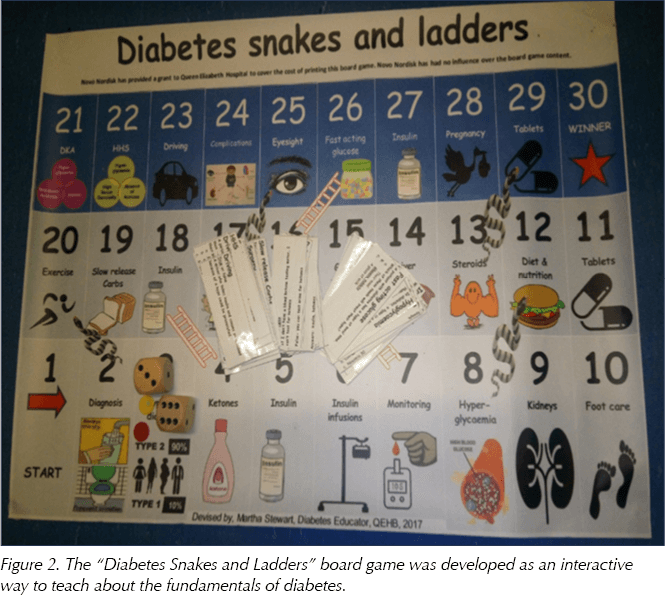
Whilst I was studying for my M.Ed, one of the areas of education that I focused on was the use of participatory activities, such as games, in the learning process. Anecdotally, nurses often comment that they find diabetes difficult to master, and so the use of games as support tools encourages interest and interaction among learners (Gaberson et al, 2015). To this end, I developed the “Diabetes Snakes and Ladders” board game (Figure 2), with funding for professional printing. The game’s main object is learning, and the snakes-and-ladders format is simply the vehicle used for this end. More details about the game are expected to be published soon.
Ward-based learning
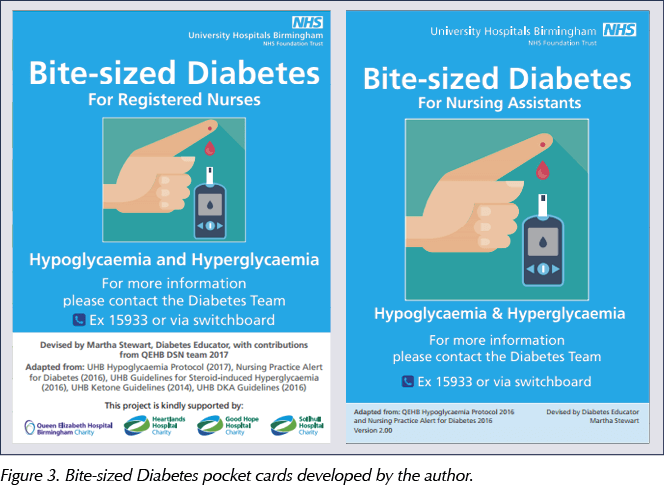
A key component of the diabetes educator role was to make ward-based diabetes learning a normal part of the nurses’ working environment. Although the diabetes clinical nurse specialists are constantly educating nurses whilst reviewing patients on the wards, the diabetes educator is a role specifically dedicated to facilitating learning in imaginative ways. I found that being conversational in educating ward nurses whilst they worked was an effective method of teaching. When new guidelines were released or if there was a spate of incidents, taking to the wards with posters and reusable learning objects supplemented the classroom sessions. One of the resources I created for ward nurses was Bite-sized Diabetes pocket cards, which work as prompts for some of the common diabetes guidelines, such as how to treat hypoglycaemia (Figure 3).
When I joined the diabetes team, I was already familiar with the concept of link nurses, and so I became involved in the diabetes link nurse project that the diabetes team had spearheaded. Although my colleagues had recruited a number of link nurses, there was not much representation across the hospital. Because my time was solely dedicated to education, I took on the task of recruiting diabetes link nurses for all clinical areas and encouraging interest in diabetes. Previous two-hourly meetings had been poorly attended because of work commitments by ward nurses. It was therefore decided to hold biannual whole-day study days, to ensure that they would not be counted in the numbers in work. The diabetes champions, as they are known, have to complete competencies adapted from the TREND-UK (2015) framework and are encouraged to disseminate good practice to their colleagues on the wards. The champions also act as our eyes and ears, highlighting both positive practice and areas that need addressing.
Another key role of the diabetes educator is utilising the key diabetes days to further the diabetes education agenda. I ensured that World Diabetes Day, Diabetes Week, Hypo Awareness Week, Insulin Safety Week and Type 2 Diabetes Prevention Week were advertised well in advance in the hospital paper (Figure 4), on screensavers and on the wards. It was a team effort to ensure that nurses, visitors and patients were engaged in education. In addition to static stands in the education centre, we often have charity events such as cycling, and we have also had a diabetes roadshow. We have had ward poster and display board competitions for the Insulin and Hypo Awareness Weeks.
One of the activities that I engage in as an educator is a ward review process called “Back to the floor”. This format was developed by a senior nurse and involves different specialities visiting wards on specified days and auditing their performance against set standards. Along with my line manager, we carry out diabetes reviews against quality outcomes around hypoglycaemia management and ketone testing, for example. Feedback is provided instantly and any relevant education is arranged. As part of evaluating the impact of education, the data captured on the visit is collated and presented at harm prevention meetings.
Evaluation of interventions
After all these interventions were introduced to improve diabetes knowledge, we needed to know whether it was all making a difference. As mentioned previously, some proxy indicators such as the voting pad data, Back to the floor data and positive learner feedback suggested that learning was occurring among nurses. More concrete quality indicators are recorded by the Quality Outcomes and Research Unit (QUORU), and the diabetes standards for nurses that we measured on Back to the floor reviews showed an improvement on the QUORU database.
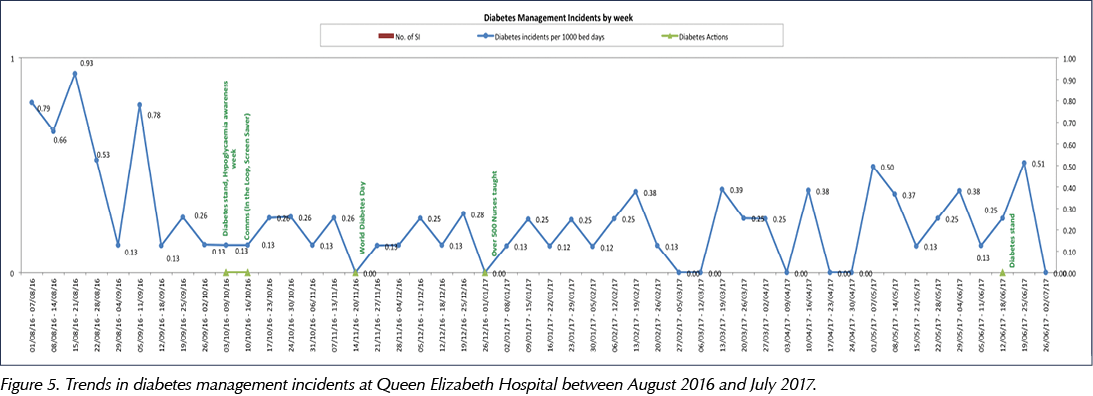
All incidents related to diabetes and/or insulin are copied to members of the diabetes team. Themes are collated through Datix analysis and Back to the floor feedback, and these feed into education. As part of the educator role, I look into the recurrent incidents and provide education at ward level to the staff involved. I created scenarios from anonymised incidents to enhance teaching sessions. The targeted teaching saw a reduction in serious incidents on the wards (Figure 5).
One of my proudest moments in the diabetes team was winning the hospital “Best in Care” award for training and education in 2017, which for me was the culmination of all the hard work in showcasing diabetes and improving staff diabetes awareness.
Moving on
At the beginning of 2018, I applied for and was appointed as a DSN in my team. My line manager valued my input in developing education in the diabetes team, and so I continue to have a role in diabetes education in the hospital. A Band 6 diabetes educator has since been employed to take on my former role, and I am one of their mentors. I have retained a number of elements from my educator role, which I juggle alongside my new DSN role. These include a strategic leadership role in diabetes education and oversight of all diabetes nursing educational initiatives; developing, promoting and overseeing novel strategies aimed at improving nurses’ diabetes knowledge and reducing diabetes-related errors; conducting virtual diabetes ward rounds; creating innovative diabetes teaching activities and resources; and delivering diabetes education sessions to nurses and medical staff in and outside the Trust. I will be further developing my DSN role by undertaking a non-medical prescribing course later this year.
Conclusion
DSNs have always had an educational role in terms of teaching staff, but they often lack the time to fully dedicate themselves to establishing a regular educational presence on the wards, creating a suite of teaching resources, and developing an overarching diabetes educational pathway and curriculum that meet the needs of workplace learning. For this reason, I believe the role of diabetes educator is an invaluable one in a diabetes team.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Julie Brake reminds us that nursing is rooted in human connection, despite our increasing reliance on technology.
11 Jun 2026