

Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic poly-peptide (GIP, previously known as gastric inhibitory polypeptide) are key incretin hormones secreted from the small intestine after oral intake of food. They lower glucose levels by stimulating insulin release from pancreatic beta-cells in a glucose-dependent fashion and by inhibiting glucagon release from the pancreatic alpha-cells. In addition, GLP-1 and GIP slow gastric emptying, reducing post-prandial glucose peaks, and suppress appetite through effects on the hypothalamus (Nauck and Meier, 2016a). Both these incretin hormones are degraded within a matter of minutes in vivo by the enzyme dipeptidyl-peptidase 4 (DPP-4).
These properties have led to the development of GLP-1 receptor agonists (RAs) and, more recently, a dual GIP/GLP-1 RA for the management of type 2 diabetes and for weight management with or without diabetes.
This article, the first of three on incretin mimetics, looks at the benefits associated with their use in type 2 diabetes. The second article considers problems, side-effects and reasons to avoid GLP-1 and GIP/GLP-1 RAs, while the third reviews their role in weight management.
Incretin mimetics for type 2 diabetes
Endogenous GLP-1 has a half-life of only a few minutes. Consequently, GLP-1 RAs were developed with molecular modifications that prolong their activity in vivo, enabling the development of once-weekly injectable preparations. Subsequent research demonstrated that GIP also plays an important role in glycaemic control in type 2 diabetes, leading to the development of the first combined single-molecule GIP/GLP-1 RA, tirzepatide (Baggio and Drucker, 2021).
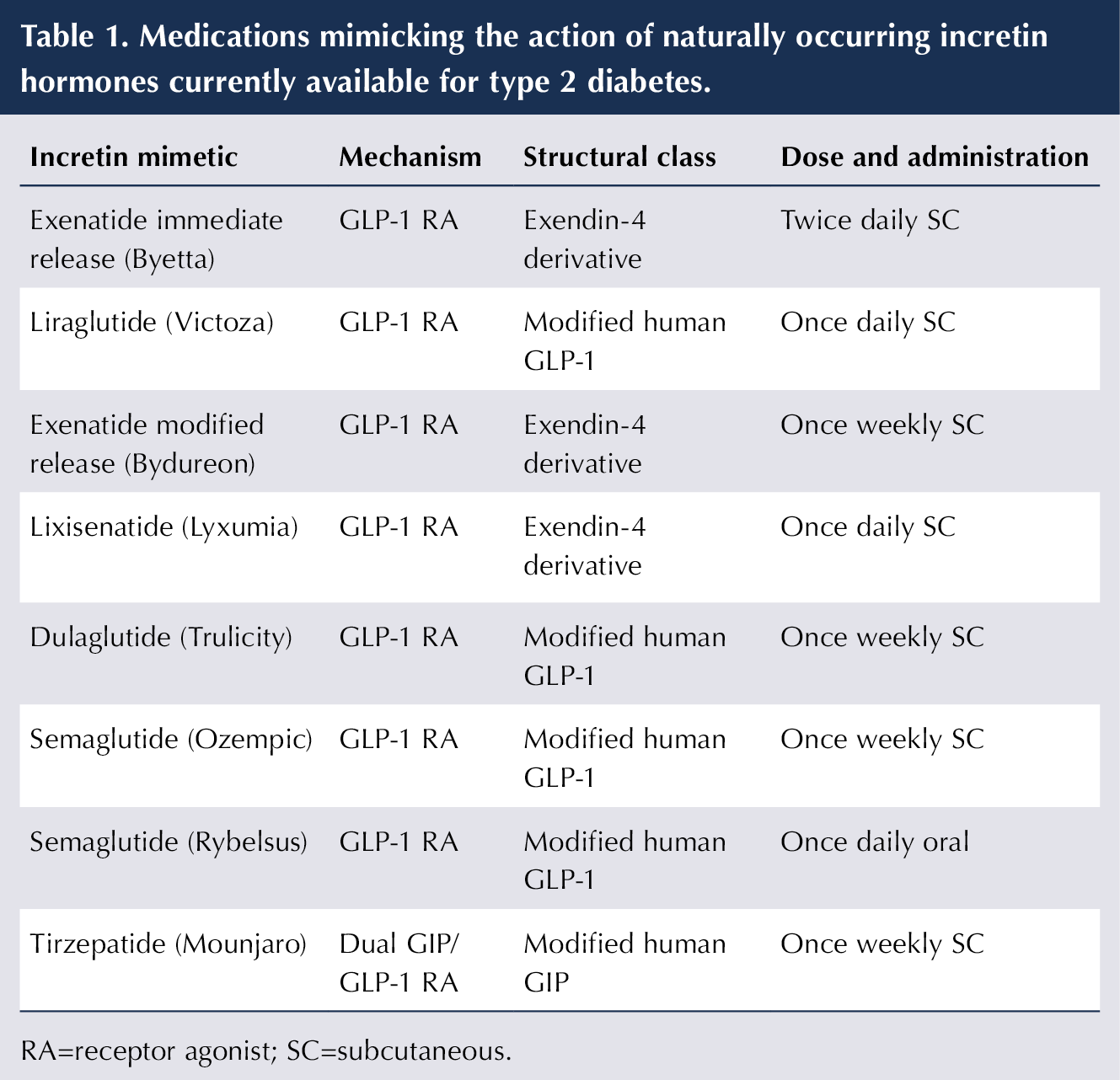
The incretin mimetics licensed for use in type 2 diabetes are summarised in Table 1 and can be divided into three structural groups.
- Exendin-4 derivatives (exenatide, lixisenatide). Their structure is based on the peptide sequence of a compound found in the saliva of the Gila monster lizard and they are resistant to degradation by the enzyme DPP-4. Exenatide modified-release (m/r) is formulated to slow its absorption. (Nauck and Meier, 2016b).
- Modified human GLP-1 analogues (liraglutide, dulaglutide, semaglutide) have close analogy to native GLP-1. Extended half-life is achieved through resistance to breakdown by DPP-4 and increasing binding affinity to plasma albumin.
- Tirzepatide is the first dual GIP/GLP-1 RA. Its structure is based on GIP but it also has amino acids in common with GLP-1. Tirzepatide has similar molecular features to the GLP-1 RAs that facilitate prolonged half-life and once-weekly administration (Nauck and D’Alessio, 2022).
Efficacy of injectable GLP-1 RAs in type 2 diabetes
GLP-1 RAs offer large improvements in HbA1c and fasting plasma glucose. Semaglutide is the most potent, achieving HbA1c reductions up to 20 mmol/mol (Pratley et al, 2018), followed by dulaglutide, liraglutide, exenatide once weekly, and lixisenatide and exenatide twice daily (Nauck et al, 2021).
An important feature of GLP-1 RA use in type 2 diabetes is weight loss, which reduces insulin resistance and typically reaches a plateau after around 6 months of treatment. Typically, weight loss is 3–7 kg at the doses used in type 2 diabetes, with semaglutide producing the greatest reduction (Nauck et al, 2021).
Oral semaglutide
GLP-1 RAs were developed as injectable therapies for type 2 diabetes because absorption of a polypeptide from the gastrointestinal tract after swallowing was considered unfeasible, as the strongly acid environment and action of peptidases in the stomach rapidly lead to its breakdown. However, the formulation of semaglutide with the absorption enhancer salcaprozate sodium (SNAC) allows small quantities of semaglutide across the gut wall, if dosing instructions are carefully followed (European Medicines Agency [EMA], 2026).
Once-daily oral semaglutide (Rybelsus) achieves an HbA1c reduction of around 11–15 mmol/mol in people with type 2 diabetes – less than injectable semaglutide but comparable to other long-acting injectable GLP-1 RAs. Weight loss is also less than injectable semaglutide, but superior to other GLP-1 RAs (Nauck et al, 2021).
Oral semaglutide offers a useful and accessible option for people with type 2 diabetes not wanting injectable therapy. The formulation has recently changed, so there is a risk of medication error – notably in the transition period when both formulations are available. The new formulation has higher bioavailability, so lower doses are required to achieve the same effect (see Box 1; EMA, 2025).
| Box 1. Dosing instructions for oral semaglutide. |
| • Starting dose, 1.5 mg od for 1 month. • After 1 month, increase to 4 mg od maintenance dose (previously 7 mg). After a further month, can be increased to 9 mg od maintenance dose (previously 14 mg). • Take on an empty stomach (overnight after fasting at least 8 hours). • Swallow with a sip of water (up to half a glass of water, 120 mL). • Wait ≥ 30 minutes before eating, drinking or taking oral medication to ensure absorption. • If there are other oral medications that are taken after an overnight fast (e.g. levothyroxine, bisphosphonates), then regimen adjustments will need to be made. • If used in combination with a sulfonylurea or insulin, consider dose reduction of these treatments to reduce risk of hypoglycaemia. |
Tirzepatide
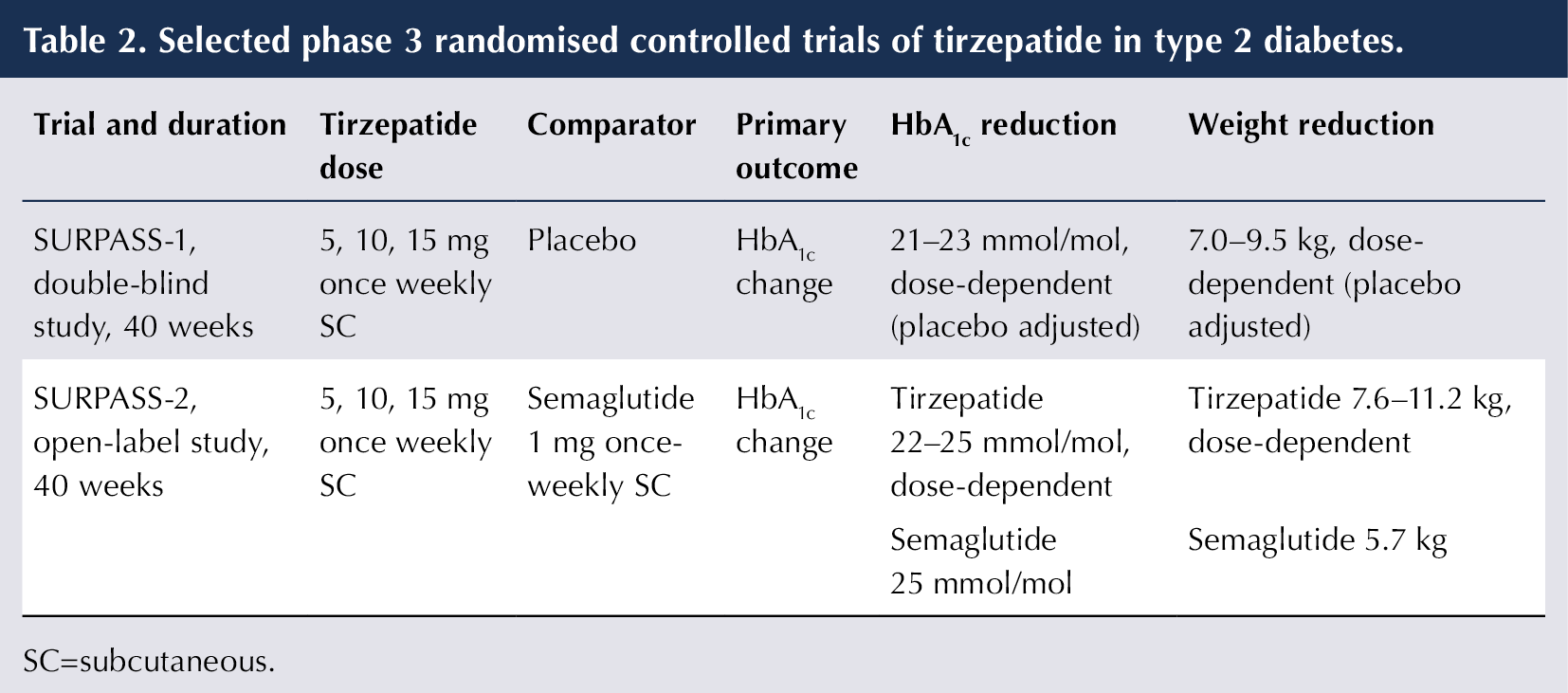
The SURPASS trials (see Table 2) established that tirzepatide achieved substantial improvements in glycaemic control and weight loss versus placebo in subjects with type 2 diabetes (Rosenstock et al, 2021). Furthermore, it outperformed semaglutide (the most potent GLP-1 RA) in both parameters (Frias et al, 2021).
Injectables: GLP-1 and GIP/GLP-1 RAs versus basal insulin
Randomised controlled trials (RTCs) have demonstrated that both semaglutide (Aroda et al, 2017) and tirzepatide (Ludvik et al, 2021; Del Prato et al, 2021) achieve greater reductions in HbA1c than long-acting basal insulin analogues, including insulin glargine and insulin degludec.
Further advantages (see Box 2) have led the American Diabetes Association (ADA) to recommend incretin mimetics as the first-choice injectable glucose-lowering therapy for type 2 diabetes, ahead of insulin (ADA, 2026). However, there are certain situations where insulin initiation should be prioritised, namely when:
- There is symptomatic hyperglycaemia (polyuria, polydipsia, weight loss).
- HbA1c is very high (≥86 mmol/mol).
- Blood glucose is very high (≥16.7 mmol/L).
- Autoimmune diabetes suspected (type 1 diabetes or latent autoimmune diabetes of adults).
| Box 2. Advantages of injectable incretin mimetics over basal insulin in type 2 diabetes. |
| • Semaglutide and tirzepatide achieve greater reductions in HbA1c level. • Weight loss (versus weight gain with insulin). • Lower risk of hypoglycaemia. • Easier dose titration. • Less blood glucose monitoring required. |
Cardiovascular protection
Randomised controlled cardiovascular outcome trials (CVOTs) have shown that liraglutide, dulaglutide and semaglutide reduce major adverse cardiovascular events (MACE; a composite of CV death, non-fatal stroke and non-fatal myocardial infarction [MI]) in people with type 2 diabetes who have established cardiovascular disease (CVD) – secondary prevention), and in those at high risk of CVD – primary prevention (Marso et al, 2016a; 2016b; Gerstein et al, 2019). The CVOT of oral semaglutide in people with type 2 diabetes and established CVD, chronic kidney disease (CKD) or both demonstrated a significant reduction in MACE compared with placebo (McGuire et al, 2025).
More recently, a CVOT compared tirzepatide with dulaglutide in people with type 2 diabetes and CVD. Given the known CV benefits of dulaglutide, placebo was not used as a comparator. Tirzepatide was non-inferior to dulaglutide in reducing CV events, supporting a CV benefit in people with type 2 diabetes (Nicholls et al, 2025).
Emerging evidence suggests that the benefits of using semaglutide (Kosiborod et al, 2023; 2024) or tirzepatide (Packer et al, 2025a; 2025b) improve functional capacity and quality of life in people with obesity-related heart failure with preserved ejection fraction, whether or not they have type 2 diabetes.
Recent final draft guidance from NICE (2026a) has recommended semaglutide – up to a dose of 2.4 mg subcutaneously once weekly – for people without diabetes and:
- with pre-existing CVD (previous MI, stroke or peripheral vascular disease)
- and a BMI of ≥27 kg/m2
for CV protection (to reduce CV death, non-fatal MI, non-fatal stroke). The recommendation is based on a trial comparing semaglutide with placebo in people with overweight/obesity with CVD but no diabetes (Lincoff et al, 2023).
Renal benefits
In the CVOTs of GLP-1 RAs in people with type 2 diabetes, composite renal outcomes (as a secondary outcome) consistently showed improvement – largely driven by reducing the progression of albuminuria.
The FLOW trial, with semaglutide in a population with type 2 diabetes and CKD, was the first RCT of GLP-1 RAs with a dedicated renal outcome. Compared with placebo, semaglutide showed improvements in both urinary albumin–creatinine ratio and rate of decline of eGFR, as well as a reduction in CV events and mortality (Perkovic et al, 2024).
Early evidence suggests that tirzepatide reduces albuminuria and attenuates the decline in eGFR in people with type 2 diabetes.
Fatty liver disease
RCTs with GLP-1 RAs, notably liraglutide and semaglutide, have demonstrated benefits in metabolic dysfunction-associated steatotic liver disease (MASLD – formerly called NAFLD). Improvements in steatosis, steatohepatitis and liver fibrosis – whether or not diabetes is present – have been identified. Tirzepatide also appears to offer improvement in hepatic steatosis (Gastadelli et al, 2022).
A recent meta-analysis reinforced that GLP-1 RA use is associated with a lower risk of liver-related complications and hepatic decompensation (Celsa et al, 2024). Incretin-based agents are not, however, licensed for the treatment of MASLD.
Updated NICE guidelines for type 2 diabetes: the place of GLP-1 RAs and tirzepatide
In previous NICE guidance for type 2 diabetes, incretin mimetics were positioned as a later option for managing hyperglycaemia – typically when triple oral therapy is ineffective, poorly tolerated or contraindicated, when BMI is sufficiently high, or when insulin needs to be avoided.
The recently updated guideline advises that incretin mimetics may be offered as part of initial triple therapy in combination with metformin m/r plus an SGLT2 inhibitor in certain situations:
- Atherosclerotic CVD. Offer subcutaneous semaglutide up to 1 mg once weekly for CV, renal and glycaemic benefits (no specific guidance on tirzepatide or oral semaglutide because CVOT results were unavailable at time of review).
- Early-onset type 2 diabetes. Consider adding either GLP-1 RA or tirzepatide, either as part of initial therapy or as first add-on, to achieve individualised glycaemic target. Early-onset type 2 diabetes (<40 years old), is an aggressive condition with high lifetime risk of CV and renal complications (NICE, 2026b).
Use of incretin mimetics as initial therapy for people with type 2 diabetes and obesity was not considered cost effective. A GLP-1 RA or tirzepatide may be considered as an add-on (to metformin plus an SGLT2 inhibitor) for glycaemic control, if initial therapy is insufficient. NICE advises using the guideline for management of overweight/obesity where this is the key consideration (NICE, 2026c).
The use of incretin mimetics for people with type 2 diabetes and CKD was also considered not cost-effective, despite evidence from the semaglutide FLOW trial. There may, of course, be individual reasons why a person with type 2 diabetes and CKD might benefit from incretin mimetics.
Further advice on using GLP-1 RAs includes:
- Stop GLP-1 RAs or tirzepatide if person becomes underweight (BMI <18.5 kg/m2), or treatment is not effective in reaching glycaemic target or weight targets and is not being used for CV benefit.
- Avoid prescribing GLP-1 RAs or tirzepatide alongside a DPP-4 inhibitor.
- Introduce drugs sequentially. For example, if triple therapy is commenced for individuals with atherosclerotic CVD, start with metformin m/r and build to the stable tolerated dose before starting an SGLT2 inhibitor. An incretin mimetic can be added once the person is stabilised on the dose of SGLT2 inhibitor.
- The incretin mimetics prioritised in the NICE guideline are liraglutide, dulaglutide, injectable and oral semaglutide, and tirzepatide.
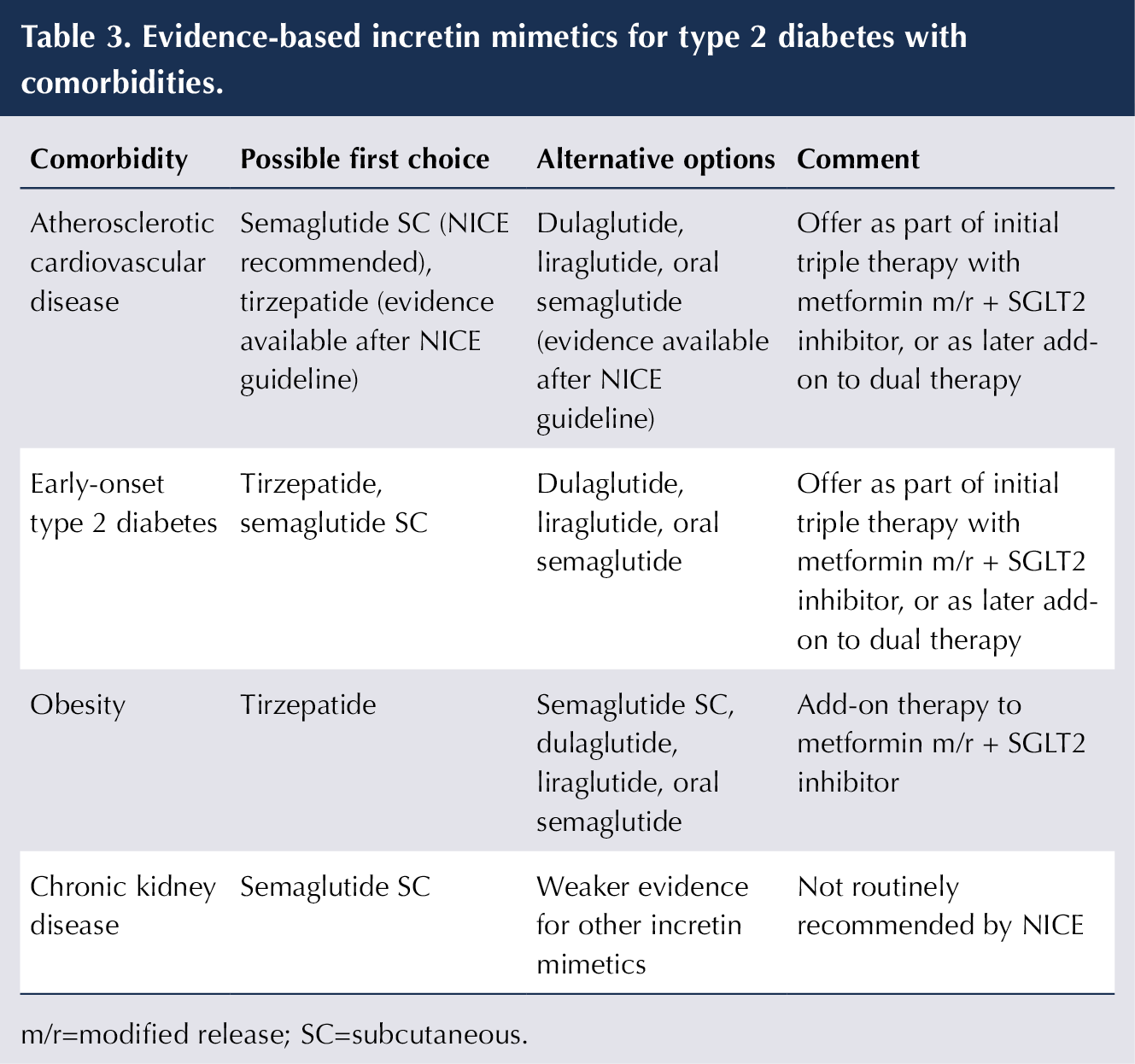
Table 3 suggests evidence-based choices for using incretin mimetics for type 2 diabetes with comorbidities. First-choice options are typically the most effective agents and are in line with options advised by NICE guidelines unless otherwise stated.
Conclusion
GLP-1 RAs are highly effective in improving HbA1c and in weight management in people with type 2 diabetes. Several preparations are available as once-weekly subcutaneous injections, with semaglutide being the most potent agent. An oral preparation of semaglutide is also available. The first-in-class dual GIP/GLP-1 RA tirzepatide, available as a once-weekly subcutaneous injection, generates even larger reductions in HbA1c and weight than semaglutide.
In people with type 2 diabetes, the incretin mimetics can reduce CV events in high-risk individuals, provide renoprotection and benefit fatty liver disease. Semaglutide and tirzepatide outperform long-acting basal insulin analogues in lowering HbA1c, and have the further advantages of lower risk of hypoglycaemia, less requirement for glucose monitoring, easier dose titration, and weight loss (rather than weight gain) with insulin.
New NICE guidelines for type 2 diabetes have advanced the priority of incretin mimetics, recommending earlier use in those with atherosclerotic CVD or early-onset type 2 diabetes. The use of incretin mimetics is also recommended as add-on therapy in people with type 2 diabetes and obesity when initial therapy provides insufficient glycaemic control.



Safety of mother and baby at centre of NICE recommendations.
8 Jul 2026